Res Dev Med Educ. 13:2.
doi: 10.34172/rdme.2024.33190
Letter to the Editor
Challenges in the educational system of maxillofacial surgery residency training in Iran: Monodisciplinarity system or dual degree system?
Arash Azarbyjani Conceptualization, Data curation, Investigation, Resources, 
Mehrdad Shahraki Project administration, Supervision, Writing – review & editing,
Sadra Amirpour Haradasht Methodology, Software, Writing – original draft, *
Author information:
Department of Oral and Maxillofacial Surgery, School of Dentistry, Zahedan University of Medical Sciences, Zahedan, Iran
Copyright and License Information
© 2024 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, as long as the
original authors and source are cited. No permission is required from the authors or the publishers.
Funding Statement
There was no funding source.
To Editor,
Oral and maxillofacial surgery, a multidisciplinary field that intersects with both medical and dental disciplines, is a branch of dentistry encompassing a variety of surgical procedures in the head and neck region. Residency training programs in this field, and their durations vary significantly across different countries, distinguishing them from other disciplines. Since the European Association for Cranio-Maxillo-Facial Surgery (EACMFS) proposed a double-degree educational program for residents in this field in 2015, there have been extensive discussions worldwide about the most appropriate educational system for oral and maxillofacial surgery residents. This article examines the current state of residency training in oral and maxillofacial surgery, discusses the challenges of monodisciplinarity versus dual disciplinarity, and offers insights into its future.
Oral and maxillofacial surgery residency in Iran
In the past 80 years, Iran has made significant advancements in this field. Currently, there is no lack of scientific knowledge among specialists in this discipline within the country. Furthermore, Iranian surgeons in this field demonstrate substantial expertise at a global level.
In Iran, individuals aspiring to this field complete their general dentistry education and pass the residency examination before embarking on a 5-year training program. This program, which includes a specialization in neurosurgery, is the longest specialized medical and dental course. Unique among dental specialties, this field requires its educational process to be conducted in hospital settings, aligning it more closely with medical specialties. As a result, residents entering this field encounter a significantly different environment, both in terms of educational discourse and patient spectrum, compared to their experience in general dentistry.1
Following the 2021 revision of the curriculum for oral and maxillofacial surgery, residents now spend two of their five-year specialized courses at a medical school during their hospital internship. This change was implemented to ensure they acquired the necessary and comprehensive medical knowledge. To further enhance their proficiency and provide additional training in medical specialties such as ophthalmology and anesthesiology, the program has integrated short-term rotations in specialized medical departments. Furthermore, residents spend another two and a half years in oral and maxillofacial surgery departments and operating rooms to develop specialized surgical skills in this field.2
Throughout their residency, residents will engage with a variety of patients and a wide range of oral and maxillofacial surgery cases. They must acquire ample experience in executing surgical procedures, diagnosing oral and maxillofacial diseases, utilizing medical equipment, and managing post-operative care.
Upon completion of their educational period, residents are expected to have acquired the following skills:
-
Diagnosing oral and maxillofacial diseases, lesions, and tissue abnormalities.
-
Administering appropriate treatment for these conditions, whether surgical or non-surgical.
-
Reconstructing soft and hard tissue in the head and neck region.
-
Performing cosmetic surgeries in the oral and maxillofacial area, including procedures such as rhinoplasty and blepharoplasty.3
Monodisciplinarity or dual disciplinarity challenges
The pathway to becoming an oral and maxillofacial surgeon can significantly vary from one country to another. In 2008, Laskin identified four global systems for training oral and maxillofacial surgeons:
-
Mode 1: Solely based on fundamental dental education.
-
Mode 2: Incorporates both medical and dental education, necessitating dual degrees in medicine and dentistry.
-
Mode 3: Involves basic medical education, which may or may not include minimal dental education.
-
Mode 4: Requires a blend of dental and medical education, but does not award a dental degree (basic medical education supplemented with dental courses).4
Oral and maxillofacial surgery became the first specialty officially recognized by the American Dental Association during the 1920s. In 1949, John Gant initiated a one-year foundational program at the University of Pennsylvania for oral surgeons, aiming to integrate the conceptual aspects of surgical education. By 1956, the Graduate Education Committee of the American Association of Oral Surgeons had established a minimum training period of three years for this specialty.
The initial planning sessions for resident education came about in 1958, culminating in the publication of the ‘Essential Foundations of the Educational Program in Maxillofacial Surgery.’ This document was reviewed and served as the inaugural plan for training oral and maxillofacial surgery residents in 1982 and 1983. During the early 1980s, the duration of oral and maxillofacial surgery residency programs was extended from three to four years.
In 1964, the American Dental Education Council approved the establishment of a commission to review advanced training in maxillofacial surgery. This led to a revision of the initial plan for resident training in oral and maxillofacial surgery in 1982 and 1983. The American Association of Oral and Maxillofacial Surgeons (AAOMS) proposed a four-year educational program, approved as the first official resident training program for oral and maxillofacial surgery on July 1, 1988.5
In the United States, residency training programs in oral and maxillofacial surgery are generally longer than those in Europe. Although the AAOMS requires a minimum of 4 years of advanced training to obtain certification in oral and maxillofacial surgery, many programs in the United States offer unified six-year residency programs that combine medical and dental education.
In America, most universities utilize the “solely based on basic dental education” system for training surgeons in this field, although many universities have embraced the double-degree system, which has been implemented in some universities.6
Currently, in Europe, two out of four residency training systems for oral and maxillofacial surgery are being implemented (Figure 1):
-
Single-degree maxillofacial surgery (with basic medical education and a minimum of 5 years of training)
-
Double-degree or dual-degree maxillofacial surgery (combining medical and dental education with a minimum of 4 years of training)
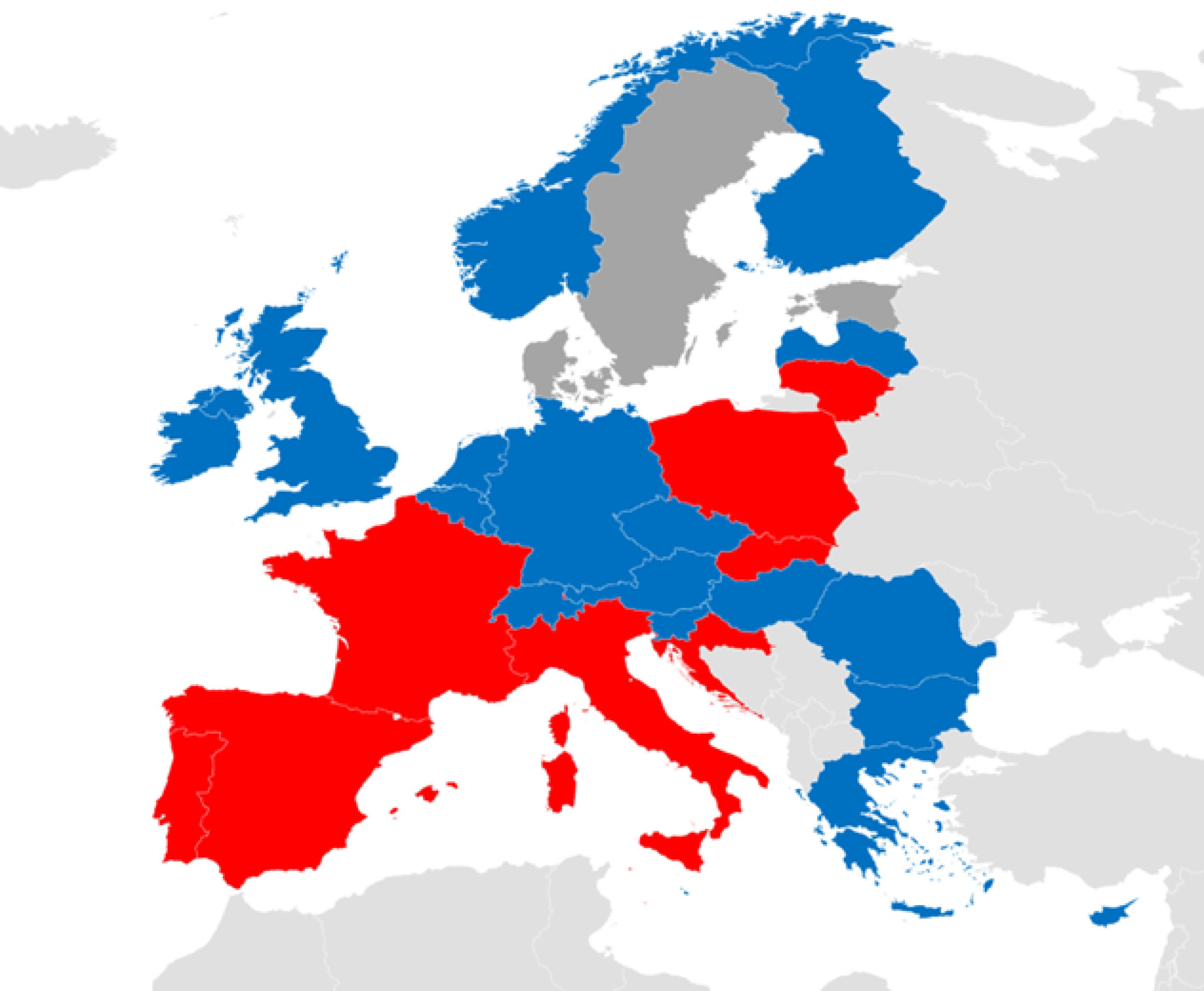
Figure 1.
Map of Europe based on the type of maxillofacial surgery residency training system. The blue color denotes the single-degree training system based on basic dental education, while the red color denotes the double-degree system
.
Map of Europe based on the type of maxillofacial surgery residency training system. The blue color denotes the single-degree training system based on basic dental education, while the red color denotes the double-degree system
A trend exists in certain countries towards transitioning from old educational systems to the double-degree system. Austria, Hungary, Luxembourg, and Bulgaria are among the countries that have recently altered their training processes.
In general, the residency training program in maxillofacial surgery comprises several components. These include theoretical courses, surgical internships, operating room attendance, commencement of supervised surgical procedures, and participation in research studies.
The residency program in this field plays a significant role in shaping the careers of specialists. It assists residents in becoming active surgeons in this field and adhering to the highest applied standards in oral and maxillofacial surgery.7
In some parts of the world, such as Canada and Australia, maxillofacial surgeons usually undergo a double-degree program. This program involves completing both dental degrees (DDS or DMD) and a medical degree (MD) before pursuing specialized training in oral and maxillofacial surgery.8
Discussions about the role of double-degree training in oral and maxillofacial surgery and the challenges in the interaction between medical and dental education systems have been ongoing for several years and remain pertinent.
Conversely, in some countries like England and many European nations, maxillofacial surgeons typically receive a medical degree (MBBS) or its equivalent and then specialize in maxillofacial surgery through supplementary training programs.
The double-degree educational program for oral and maxillofacial surgery was first proposed in 2015 by the EACMFS. This proposal aimed to establish a standardized educational program that provides residents in this field with a comprehensive understanding of the medical and dental aspects of their discipline.9,10
There are numerous reasons for implementing the double-degree educational program for residents, including:
-
Broader knowledge: The double-degree program provides residents in oral and maxillofacial surgery with a more comprehensive education. This allows them to gain deep knowledge in both dental assistance and maxillofacial surgery, enabling them to perform their duties with greater expertise.
-
Improved patient care: With a double-degree program, residents in oral and maxillofacial surgery will be better prepared to provide high-quality care to patients and have a deeper understanding of patient conditions.
-
Increased job opportunities: Maxillofacial surgeons with two degrees will have numerous advantages in the job market and will expand their career choices.
-
Professional advancement: Holding a double degree can open up opportunities for professional growth and advancement in the field of oral and maxillofacial surgery. By offering a double-degree educational program, educational institutions can ensure that residents in this field acquire the latest knowledge and necessary skills.
-
Effective collaboration with other specialists: Maxillofacial surgery often involves collaboration with other medical specialists. A double-degree program can facilitate more effective communication and collaboration among specialists, leading to improved patient treatment success.
-
Standardization of residents’ training programs: Implementing a double-degree educational program can help standardize the education provided to residents in oral and maxillofacial surgery in different regions, ensuring that all graduates have similar levels of knowledge and skills, thereby enhancing patient care quality.11,12
According to the results of these studies, double-degree training in oral and maxillofacial surgery has resulted in increased efficiency among specialists in this field. Furthermore, these programs enable residents to gain experience in two different educational environments and become familiar with new and advanced treatment methods.
Some researchers believe that double-degree education in oral and maxillofacial surgery is an appropriate solution for increasing specialization and efficiency in this field, especially as the interaction between dental and medical fields in oral and maxillofacial surgery solidifies the position and role of this discipline. Therefore, its development and promotion on a global scale should be given attention.13
Another group of experts accentuates the increased proficiency in medicine and dentistry and argues that separate degrees allow residents to acquire deeper knowledge in each field. They believe that this specialization leads to better patient care and outcomes.
On the other hand, having a double degree can provide more specialized training, allowing residents to delve deeper into specific medical and dental areas. This can be beneficial for those who wish to focus on specific aspects of oral and maxillofacial surgery or pursue academic careers where specialized knowledge is highly valuable.11
Certainly, the double-degree educational system will entail a longer study period compared to the one-degree system and will present a more rigorous yet comprehensive curriculum. Naturally, holding a double degree will expand the scope of operation and surgery for maxillofacial surgeons. It is worth mentioning that concurrently holding medical and dental degrees creates more job opportunities and research prospects due to broader knowledge for maxillofacial surgeons.10
Overall, proposing and implementing a double-degree educational program for oral and maxillofacial surgery residents will be beneficial for both individuals pursuing this career path and the patients they serve. It enhances their knowledge, skills, career prospects, and professional growth while improving patient care.
In fact, providing a definitive answer as to whether the training of oral and maxillofacial surgery residents should be a one-degree or double-degree system is challenging. However, we can analyze the information presented to understand different perspectives.
Advocates of the one-degree system argue that a single degree for maxillofacial surgery specialization exists. It emphasizes the importance of comprehensive education in medicine and dentistry, as maxillofacial surgeons must have a deep understanding of both fields. They suggest that combining these disciplines in a comprehensive program ensures complete education and better prepares surgeons for the complexities of their profession.12,14
Considering these perspectives, it becomes clear that there are valid arguments for both the one-degree and double-degree systems in the training of oral and maxillofacial surgery residents. A unified educational program can provide a holistic approach and ensure a strong foundation in medicine and dentistry. This can be beneficial for surgeons whose aim is to have a broad understanding of their field and provide comprehensive patient care.
Ultimately, the decision about whether the training of oral and maxillofacial surgery residents should be in what form may depend on various factors such as educational objectives, available resources, and professional preferences. It is important for stakeholders in this field to carefully consider these factors when designing residency programs that meet the future needs of maxillofacial surgeons.
Acknowledgments
We would like to express our sincere gratitude for the invaluable support received from the Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Zahedan University of Medical Sciences especially Dr. Shahab Farshad. Their assistance and guidance have been crucial in the successful completion of this study.
Competing Interests
The authors declare no conflict of interest.
Ethical Approval
Not applicable.
References
- Yarmoradian S, Shahraki M, Amirpour Haradasht S. A brief history of oral and maxillofacial surgery in Iran. J Res Hist Med 2023; 12(2):145-8. [ Google Scholar]
- behdasht.gov. Approved Educational Programs for Oral and Maxillofacial Surgery in Iran: Secretariat of Dental and Specialized Education Council. Updated 2018. Available from: https://gpde.behdasht.gov.ir/Takhasos_Dandan.
- Walker TW, Cascarini L, Brennan PA. Educational paper: research in oral and maxillofacial surgery. Br J Oral Maxillofac Surg 2010; 48(8):629-32. doi: 10.1016/j.bjoms.2009.10.007 [Crossref] [ Google Scholar]
- Kumar S. Training pathways in oral and maxillofacial surgery across the globe-a mini review. J Maxillofac Oral Surg 2017; 16(3):269-76. doi: 10.1007/s12663-017-1020-0 [Crossref] [ Google Scholar]
- Felsenfeld AL, Casagrande A. Oral and maxillofacial surgery residency education. J Calif Dent Assoc 2004; 32(10):817-22. doi: 10.1080/19424396.2004.12224029 [Crossref] [ Google Scholar]
- Payne KFB, Higginson J, Basyuni S, Goodson AMC, Chadha A, Elledge R. Academic training in oral and maxillofacial surgery - when and how to enter the pathway. Br J Oral Maxillofac Surg 2023; 61(2):124-30. doi: 10.1016/j.bjoms.2023.01.003 [Crossref] [ Google Scholar]
- Ren YF. [Oral and maxillofacial surgery residency training in the United States: what can we learn]. Zhonghua Kou Qiang Yi Xue Za Zhi 2017; 52(4):218-22. doi: 10.3760/cma.j.issn.1002-0098.2017.04.005 [Crossref] [ Google Scholar]
- McKechnie A, McCaul J. Research training for oral and maxillofacial surgery. Br J Oral Maxillofac Surg 2007; 45(6):478-83. doi: 10.1016/j.bjoms.2006.11.015 [Crossref] [ Google Scholar]
- Magennis P, Hölzle F, Ulrich HP, Acero J, Hutchison I. The specialty of oral and maxillofacial surgery (OMFS) in Europe – part 2: training environment including the new Union of European Medical Specialists (UEMS) Oral and Maxillofacial Surgery European Training Requirement (OMFS ETR). Br J Oral Maxillofac Surg 2022; 60(10):1340-6. doi: 10.1016/j.bjoms.2022.09.011 [Crossref] [ Google Scholar]
- Oral and Maxillo-Facial Surgery Section of UEMS. About OMFS in Europe. 2023. Available from: https://omfsuems.eu/about_omfs_europe/default.aspx.
- Kaban LB, Perrott DH. Dual-degree oral and maxillofacial surgery training in the United States: “back to the future”. J Oral Maxillofac Surg 2020; 78(1):18-28. doi: 10.1016/j.joms.2019.08.026 [Crossref] [ Google Scholar]
- Meyer RA, Bagheri SC. Double degree training supported. J Oral Maxillofac Surg 2010; 68(7):1703-4. doi: 10.1016/j.joms.2010.04.001 [Crossref] [ Google Scholar]
- Ganjawalla KP, Jazayeri HE, Moe JS, Tannyhill RJ. Dual degree training: balancing clinical aptitude and medical licensure requirements. J Oral Maxillofac Surg 2021; 79(10):1988-90. doi: 10.1016/j.joms.2021.04.032 [Crossref] [ Google Scholar]
- Stoelinga PJ. International guidelines for specialty training in oral and maxillofacial surgery. Int J Oral Maxillofac Surg 1992; 21(3):130-2. doi: 10.1016/s0901-5027(05)80777-5 [Crossref] [ Google Scholar]