Res Dev Med Educ. 14:33267.
doi: 10.34172/rdme.025.33267
Original Article
Effectiveness of a short course in communication skills for medical doctors: Evaluation based on a one group pretest posttest design
Masumeh Abdi Conceptualization, Data curation, Methodology, Resources, Writing – original draft, Writing – review & editing, 1 
Amin Beigzadeh Conceptualization, Data curation, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing, 2, *
Ali Asghar Hayat Conceptualization, Data curation, Investigation, Methodology, Project administration, Software, Supervision, Writing – original draft, Writing – review & editing, 2
Mohammad Hasan Keshavarzi Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, 2
Habibolah Rezaei Conceptualization, Data curation, Methodology, Project administration, Software, Supervision, Writing – original draft, Writing – review & editing, 3, *
Author information:
1Clinical Education Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
2Education Development Center, Sirjan School of Medical Sciences, Sirjan, Iran
3Cellular and Molecular Research Center, Yasuj University of Medical Sciences, Yasuj, Iran
Abstract
Background:
Effective communication skills are crucial in healthcare, particularly in the clinical setting where interactions often occur under high stress. This study aimed to identify the educational needs of medical doctors, design a communication skills course, and evaluate its impact on their performance at Yasuj University of Medical Sciences in 2022.
Methods:
A quasi-experimental, one-group pretest-posttest design was employed involving 196 participants, including medical doctors, nursing staff, and medical students. Intervention consisted of 9 h of communication skill training, containing theory/debriefs and practical group sessions with role-plays. A self-developed questionnaire assessed communication competencies before and after a three-session course focused on enhancing communication skills. Also, perceptions of medical doctors were elicited using content analysis method.
Results:
Pretest and posttest comparisons revealed significant improvements in several areas, notably in active listening (e.g., "Let the patient finish his/her speech without interrupting" increased from 3.40 to 4.43, P<0.001) and verbal feedback skills (e.g., "Give negative feedback at the right time" improved from 2.95 to 3.68, P=0.016). However, areas such as patient engagement and the use of visual aids showed mixed results, indicating ongoing training is necessary. Overall, participants reported high satisfaction with the course, achieving a mean score of 3.98. Furthermore, the course was deemed valuable due to its relevance to the workplace and its significant influence on performance outcomes.
Conclusion:
The communication skills course effectively addressed critical gaps in medical doctors’ communication abilities, enhancing their interactions with patients and colleagues. These findings underscore the importance of integrating continuous communication training into medical education to improve patient outcomes and foster collaborative team dynamics in the clinical settings. Future research should investigate the long-term effects of such training interventions.
Keywords: Communication skills, Medical doctors, Medical education, Quasi-experimental
Copyright and License Information
© 2025 The Author(s).
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, as long as the original authors and source are cited. No permission is required from the authors or the publishers.
Funding Statement
This research was financially supported by the Research Deputy of Shiraz University of Medical Sciences.
Introduction
Communication skills encompass the behaviors and actions that facilitate effective interaction with others, fostering positive responses and minimizing the likelihood of adverse reactions.1 The significance of effective communication skills in human life cannot be overstated. Human potential flourishes primarily within the context of interpersonal relationships, which are essential for fostering mental health, personal growth, identity formation, enhanced job performance, adaptability, and self-actualization.2,3
Concerning the clinical environment, the significance of communication skills has been underscored in the clinical settings, particularly given the presence of patients in critical conditions.4 It is essential for medical doctors and nursing staff within these environments to cultivate rapport not only with patients, but also with students. Consequently, possessing the requisite communication skills is of paramount importance.5-7 A considerable portion of medical students’ education is allocated to clinical training. In this context, medical doctors assume a crucial role, with their communication skills being among the most impactful factor.8 Consequently, the acquisition of communication skills is evidently a vital component of their responsibilities.9
Research suggests that effective communication skills are advantageous for medical doctors, students, and patients alike. Students who maintain a positive rapport with their medical teachers tend to demonstrate increased motivation and effort in their academic pursuits.10 Enhanced relationship correlates with increased student confidence, support, and motivation to learn, which in turn enhances the overall quality of education.11,12 In addition, the medical teacher has the ability to enhance the learning process fostering effective communication, thereby improving teaching efficacy while upholding the respect and admiration of the students.13,14 In a similar line, effective communication skills yield significant advantages for patients. Through communication, patients articulate their experiences of pain and illness, presenting accurate descriptions of their conditions and histories. This leads to improved diagnoses, treatment outcomes, and overall satisfaction with the healthcare services received.15-17
Numerous studies have been undertaken regarding the communication skills of teachers. The study conducted by Rezaian et al. concluded that the communication skills of teachers was at a moderate level, indicating a need for enhanced training programs.18 In another study carried out by Yazdani et al, findings demonstrated that teachers can enhance the quality of their teaching by refining their verbal communication skills and feedback mechanisms. The significance of communication skills, particularly in the realm of feedback, plays a crucial role in augmenting teaching effectiveness.19 Various research studies emphasize the significance of implementing communication skills courses or conducting workshops for medical doctors, particularly when integrated into a continuous professional development framework.20,21
Given the importance of effective interpersonal communication in the clinical environment, communication skills training is an important issue in medical schools, and great emphasis has been put on its acquisition based on the training program of medical students.22,23 Therefore, due to the importance of this skill in the clinical setting, and due to the lack of research in this regard at Yasuj University of Medical Sciences, this study was conducted with these objectives: 1) to identify the educational needs of medical doctors, 2) to design a communication skills course, 3) to evaluate its impact on performance, and 4) to elicit medical doctors’ perceptions of the communication skills course.
Methods
Study setting and participants
This quasi-experimental study (one-group pretest-posttest design) was carried out at educational hospitals affiliated with Yasuj University of Medical Sciences, in the year 2022. The study sample comprised three groups: 1) medical doctors; 2) medical students; and 3) nursing staff. Participants were recruited by convenience sampling method, which is a non-probability sampling technique. This approach was chosen due to its practicality and the accessibility of the target population within the educational hospitals affiliated with Yasuj University of Medical Sciences. Specifically, potential participants were approached and informed about the study’s objectives, procedures, and the voluntary nature of participation. The demographic characteristics of the participants are presented in Table 1.
Table 1.
The demographic information of the three batches of participants
|
Variables
|
|
Medical doctors
|
Nursing staff
|
Students
|
|
Interns
|
Residents
|
| Age (Mean ± SD) |
43.1 ± 6.05 |
33.66 ± 5.51 |
26.25 ± 2.5 |
36.33 ± 3.7 |
| Gender |
Male (No.) |
22 |
6 |
14 |
9 |
| Female (No.) |
30 |
86 |
18 |
11 |
| Teaching experience (Mean ± SD) |
9.59 ± 5.43 |
- |
- |
- |
| Nursing experience (Mean ± SD) |
- |
9.43 ± 5.5 |
- |
- |
Inclusion and exclusion criteria
The criteria for including medical doctors in the study were as follows: A) willingness to participate in the study, B) involvement in both pretest and posttest evaluations, C) attendance in the communication skills training course, and D) a minimum of three years of teaching experience in the clinical environment.
The inclusion criteria for medical students encompassed: A) willingness to engage in the study, B) participation in clinical rotations within the clinical setting over the preceding year, and C) successful completion of both pretest and posttest evaluations.
The inclusion of nurses in the study was contingent upon several criteria: A) a willingness to engage in the study, B) employment as nursing staff within the clinical department, C) a minimum of three years of professional experience in the clinical departments, D) regular collaboration with medical doctors in the clinical setting, and E) successful completion of both pretest and posttest evaluations.
Participants were excluded from the study for several reasons, including their failure to complete the questionnaires, providing incomplete responses to at least 10% of the items, expressing a lack of willingness to participate, and having previously engaged in a communication skills course.
Baseline needs assessment
To evaluate the communication skills of medical doctors, an initial assessment was performed using a pre-test designed to measure these competencies. Data collection involved the distribution of a self-developed questionnaire to medical doctors, nursing staff, and medical students. Similarly, a post-test utilizing the same measurement items was administered following the completion of the short course focused on enhancing communication skills. Participants were briefed on the purpose of the study and any ambiguities was explained to them. It is noteworthy to indicate that the posttest evaluation was carried out three months following the implementation of the communication skills course. This interval was necessary to facilitate the instruction of medical students during their clinical rotations and to foster interactions between medical doctors and nursing staff.
Intervention (course design)
The communication skills training course for medical doctors consisted of three sessions, each lasting three hours, for a total duration of nine hours. The sessions were conducted over a span of three consecutive weeks to ensure manageable participation for the medical doctors, accommodating their demanding schedules. Each session was designed to build upon the previous one, allowing for progressive development of communication skills through a structured curriculum. The training course was conducted at a suitable time within the facilities of Martyr Dr. Jalil hospital. Medical doctors were informed ahead of time to accommodate their participation, considering their demanding daily responsibilities. In addition, they were informed about the study objectives. Oral consent was granted from participants. The short course featured distribution of theoretical instruction and collaborative activities, including role-playing exercises through a scenario-based approach, followed by comprehensive debriefing sessions after each group activity. All the three sessions were conducted with the present of a psychologist specialist, two clinical specialists, and a medical education specialist. It is noteworthy to highlight that this course has been authorized by the Continuing Medical Education department at Yasuj University of Medical Sciences. The content covered of the course is detailed in Table 2.
Table 2.
Content of the communication skills course tailored for medical doctors
|
Objective: Effective communication skills to improve patient care and team collaboration
|
|
Item
|
sessions
|
topics
|
| Theoretical content |
Session 1 |
Introduction to communication skills in the clinical setting
Active listening
-
Attention: Techniques to maintain focus during high-stress situations.
-
Empathy: Understanding and acknowledging patient emotions.
-
Clarification: Asking questions to ensure understanding.
-
Reflection: Paraphrasing to confirm comprehension.
Verbal communication
|
| Theoretical content |
Session 2 |
Nonverbal Communication
Patient center
Emotion control
|
| collaborative activities |
Session 3 |
Role-playing scenarios and group work to:
-
Practice active listening
-
Provide feedback to enhance communication skills
-
Verbal and nonverbal communication in high-stress situations
-
Emotion control in high-stress situations
|
We recognize the importance of monitoring both instructor adherence and participant engagement to accurately interpret variations in outcomes. To address this, we implemented several strategies during the course delivery. Instructors were provided with a structured curriculum and were encouraged to follow it closely, with periodic check-ins to ensure adherence to the planned content. Additionally, participant engagement was monitored through attendance records and active participation in role-playing exercises and discussions. Feedback forms were also collected after each session to gauge participant involvement and satisfaction. Moving forward, we will emphasize the inclusion of fidelity measures in our future studies to enhance the reliability of our findings and better understand the impact of the intervention.
Pretest-posttest instrument
To ascertain the specific areas requiring enhancement in communication skills among medical doctors, and to develop a concise communication skills course, a questionnaire was designed by the researchers. This questionnaire was developed based on the existing literature,24-26 and is divided into two sections. The initial section consists of demographic variables such as age, gender, teaching experience (specifically for medical doctors), and professional nursing experience (specifically for nursing staff). The subsequent section focuses on communication competencies, featuring 4 items associated with listening abilities, 13 items addressing verbal communication, 8 items related to non-verbal communication, 14 items concerning patient-centered, 11 items that pertain to emotion control, and 17 items that explore the dynamics of teacher-student relationships. Based on this questionnaire, participants are required to score items on a 5-point Likert scale ranging from never (1 score) to always (5 scores). Scores 0-1.25, 1.26-2.5, 2.6-3.75, and 3.75-5 show weak, moderate, good, and strong communication skills, respectively. All the items of the questionnaire that were rated lower than strong level was considered as requiring improvement actions.
Validity and reliability of the instrument
To ensure the validity of the questionnaire, a panel consisting of four medical specialists, one specialist in medical ethics, and two experts in medical education evaluated both the face and content validity of the instrument (content validity ratio [CVR] and content validity index [CVI]). The CVR and CVI for all items were 1. For reliability purposes, the questionnaire was administered to 16 participants over a span of two weeks, employing the test-retest reliability method. The calculated Cronbach’s alpha was 0.77, which signifies an acceptable level of reliability.
The satisfaction questionnaire
The evaluation of the course was conducted using two levels of the Kirkpatrick model,27 specifically focusing on satisfaction and learning outcomes. To gauge participant satisfaction, a researcher-designed questionnaire was developed to measure the participants’ contentment with the study intervention upon its conclusion. This instrument consists of 10 items with responses recorded on a five-point Likert scale, where a score of 5 indicates strong agreement and a score of 1 indicates strong disagreement. In addition, participants were invited to articulate their perceptions of the course through an open-ended inquiry. The CVR and CVI for the quantitative items in this questionnaire were both established at 1. Furthermore, the reliability of the questionnaire, assessed through Cronbach’s alpha, was determined to be 0.78. In terms of learning, the pre-test and post-test assessment measures were compared accordingly. The research framework is depicted in Figure 1.
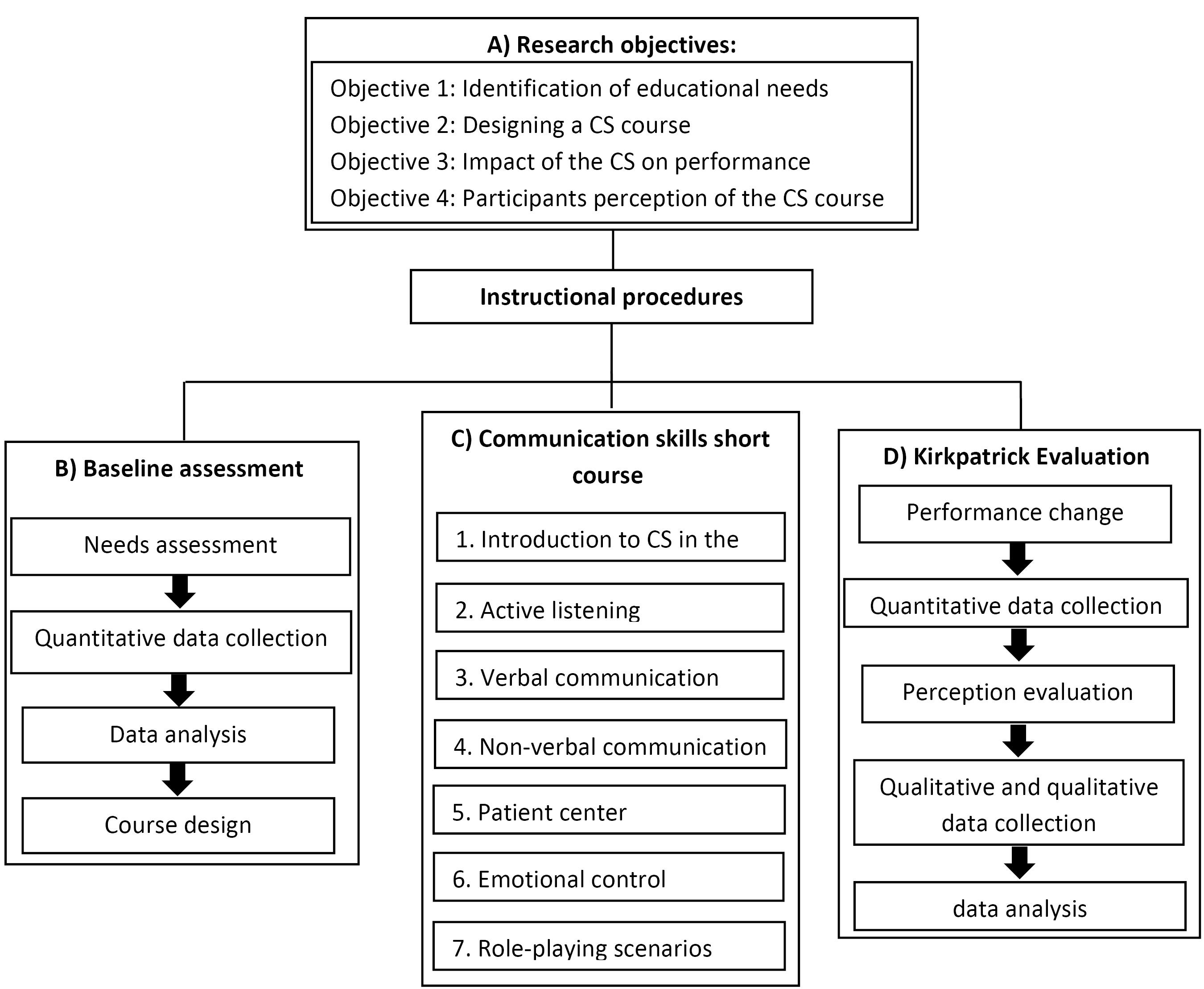
Figure 1.
Research framework and instructional procedures
.
Research framework and instructional procedures
Data analysis
The analysis of the data involved the application of descriptive statistics, specifically the mean and standard deviation, alongside inferential statistical tests. In this context, a paired t-test was performed to evaluate the differences in scores recorded prior to and following the intervention. Data analysis was conducted by SPSS software version 26 and P< 0.05 was considered as statistically significant.
The open-ended inquiry was analyzed using summative content analysis. This methodological approach is frequently employed for analyzing open-ended survey responses. This technique involves the identification of key terms, which may be quantified as needed in accordance with the study’s objectives, in order to gain insights into the situation at hand.28 Two researchers (AB, and HR) conducted an independent analysis of the text by reading and re-reading it to extract key terms from the responses. These terms were subsequently organized into distinct categories. This methodology was deemed the most appropriate given that the responses were primarily in single word and short sentence formats. The established categories were then subjected to discussion to ensure their validity.
Ethical considerations
All participants were informed that their involvement in the study was entirely voluntary, and they could withdraw at any time without any impact on their professional relationships or responsibilities. We ensured that the recruitment process was conducted by individuals not directly involved in the participants’ clinical supervision to mitigate any power dynamics. Additionally, we implemented measures to maintain confidentiality and anonymity throughout the study. There were no conflicts of interest reported by the research team, and we are committed to upholding the highest ethical standards in our research practices.
Results
Totally, 196 participants took part in this study. The study participants included a diverse group comprising medical doctors (n = 52, 26.53%), nursing staff (n = 92, 46.94%), and students (n = 52, 26.53%), specifically interns and residents. Concerning the age variable, the mean age of medical doctors was 43.1 years (SD = 6.05), while nursing staff had a mean age of 33.66 years (SD = 5.51). Interns were the youngest group with a mean age of 26.25 years (SD = 2.5), followed by residents with a mean age of 36.33 years (SD = 3.7). In terms of gender distribution, in the medical doctors’ group, there were 22 males and 30 females, indicating a female majority of approximately 57.7%. The nursing staff showed an even more pronounced gender disparity, particularly among interns, where females dominated with 86 compared to only 6 males, reflecting a striking 93.5% female representation. The residents maintained a more balanced ratio with 14 males and 18 females, resulting in about 43.8% male representation. Regarding experience, medical doctors had an average teaching experience of 9.59 years (SD: 5.43), highlighting their educational background, but nursing staff reported an average nursing experience of 9.43 years (SD: 5.5).
Table 3 depicts the comparison of pre-test and post-test assessment on the communication skills of medical doctors. Findings revealed a generally positive assessment before the intervention, with most items scoring above 3.75. However, several items indicated areas for potential improvement, particularly those scoring below this threshold. The pretest scores for active listening skills among medical doctors varied, with most items scoring above 4.0, indicating a generally positive self-assessment. However, some items revealed opportunities for improvement. Notably, “Let the patient finish her speech without interrupting her” scored 3.40, suggesting that medical doctors may struggle with allowing patients to express themselves fully before responding. For verbal and non-verbal skills, the item “Give negative feedback at the right time” received a score of 2.95, highlighting a lack of confidence in delivering timely constructive feedback. Similarly, “Describe others’ behavior without judgment” scored 3.05, suggesting difficulties in providing objective feedback. Other items, such as “Welcome the patient” (3.16), and “Explain treatment processes to the patient in sufficient detail” (3.17) indicated a need for enhancement in creating a welcoming environment and ensuring clear communication of treatment processes. These scores underscore the importance of the clinical communication skills course in addressing these specific areas and improving overall communication effectiveness among medical doctors. By the same token, the item “Use visual aids like diagrams and written information when communicating with the patient” stood out with a notably low score of 2.89, reflecting a significant opportunity for improvement. This low score suggests that medical doctors may not effectively utilize visual aids, which are crucial for enhancing patient understanding and engagement. For patient-centered items, only the item, “Ask the patient to restate the information in his/her own words and clarify any errors” received a low score of 3.09, suggesting that medical doctors may struggle to ensure patients fully understand the information provided, which is essential for effective communication. The last but not least, for emotional control items, the item “Accept patient’s positive feedback without embarrassment” received a notably low score of 3.27, indicating a significant area for improvement. This score suggests that medical doctors may struggle to accept and acknowledge positive feedback from patients, which is essential for building trust and rapport.
Table 3.
Comparing the communication skills of medical doctors before and after the implementation of the clinical communication skills course
|
Items
|
Pretest
|
Posttest
|
statistics
|
df
|
P
value
|
|
Active listening (4 items)
|
| Show interest in listening to the patient. |
4.47 |
4.51 |
0.51 |
194 |
0.61 |
| Let the patient finish his/her speech without interrupting. |
3.40 |
4.43 |
0.42 |
194 |
0.66 |
| Allow the patient time to think before responding or to continue speaking after a brief pause. |
4.39 |
4.35 |
0.56 |
194 |
0.57 |
| Verbally or non-verbally, facilitate the patient's responses. |
4.33 |
4.31 |
0.31 |
194 |
0.75 |
|
Verbal skill (13 items)
|
| Greet the patients. |
4.56 |
4.56 |
0.89 |
194 |
0.92 |
| Welcome the patient. |
3.16 |
4.22 |
0.71 |
194 |
0.47 |
| Provide explanation to the patient in an organized manner. |
4.29 |
4.27 |
0.22 |
194 |
0.82 |
| Explain treatment processes to the patient in sufficient detail. |
3.17 |
4.24 |
0.82 |
194 |
0.41 |
| Use follow-up questions when talking to the patient. |
4.48 |
4.30 |
0.81 |
194 |
0.41 |
| Refuse to ask multiple questions at the same time. |
4.33 |
4.29 |
0.69 |
194 |
0.48 |
| If the patient appears confused, speaks more calmly. |
4.31 |
4.44 |
1.73 |
194 |
0.08 |
| Avoid giving advice, information, or premature reassurance. |
4.21 |
4.30 |
0.81 |
194 |
0.41 |
| Use specific examples to answer the patient's questions. |
4.21 |
4.25 |
0.46 |
194 |
0.64 |
| Provide positive feedback to boost others' confidence. |
4.24 |
4.22 |
0.36 |
194 |
0.71 |
| Give negative feedback at the right time. |
2.95 |
3.68 |
2.44 |
194 |
0.016 |
| Describe others' behavior without judgment. |
3.05 |
3.75 |
2.37 |
194 |
0.019 |
| Summarize the patient's statements to ensure students understand them correctly. |
4.23 |
4.21 |
0.28 |
194 |
0.77 |
|
Non-verbal skills (8 items)
|
| Strive to be respectful in conversations with the patient. |
4.46 |
4.49 |
0.41 |
194 |
0.67 |
| Maintain eye contact with patient and avoid turning away. |
4.41 |
4.48 |
0.72 |
194 |
0.47 |
| Greet the patient with an open mind at the first meeting. |
4.47 |
4.47 |
0 |
194 |
1 |
| Avoid being defensive when speaking with the patient. |
4.40 |
4.36 |
0.55 |
194 |
0.58 |
| Aim for the right tone of voice when speaking to the patient. |
4.49 |
4.40 |
1.35 |
194 |
0.17 |
| In case of doing many things and to ensure good communication with the patient, interruption is avoided. |
4.32 |
4.29 |
0.32 |
194 |
0.74 |
| Use visual aids like diagrams and written information when communicating with the patient. |
2.89 |
4.05 |
1.49 |
194 |
0.13 |
| Recognize and acknowledge the patient's non-verbal cues. |
4.21 |
4.19 |
0.28 |
194 |
0.77 |
|
Patient-centered (14 items)
|
| Talk to the patient about treatment options. |
4.39 |
4.40 |
0.14 |
194 |
0.88 |
| Provide honest explanations of treatment options, outlining pros and cons. |
4.33 |
4.41 |
0.92 |
194 |
0.35 |
| Explain the expected outcome and the disease's short- and long-term consequences. |
4.32 |
4.34 |
0.29 |
194 |
0.76 |
| Ask permission from the patient for a physical examination. |
4.34 |
4.33 |
0.17 |
194 |
0.86 |
| Discuss the treatment results with the patient to assess satisfaction and adherence. |
4.34 |
4.41 |
0.99 |
194 |
0.32 |
| Maintain the patient's dignity throughout the examination. |
4.53 |
4.47 |
0.79 |
194 |
0.43 |
| Ask the patient about her beliefs about problems. |
4.22 |
4.37 |
1.92 |
194 |
0.05 |
| Consider the patient's cultural background and abilities during treatment. |
4.24 |
4.29 |
-0.55 |
194 |
0.58 |
| Ask the patient about her concerns. |
4.15 |
4.07 |
0.82 |
194 |
0.40 |
| Ask the patient about her expectations. |
4.13 |
4.11 |
0 |
194 |
1 |
| Encourage the patient to ask questions. |
4.26 |
4.13 |
1.67 |
194 |
0.09 |
| Assess the patient's knowledge of disease and ask how much more information is needed. |
4 |
4.07 |
-0.81 |
194 |
0.41 |
| Ask the patient to restate the information in his/her own words and clarify any errors. |
3.09 |
4.17 |
-0.98 |
194 |
0.32 |
| Summarize the session and clarify the care plan. |
4.18 |
4.15 |
0.35 |
194 |
0.72 |
|
Emotion control (11 items)
|
| Remain aware of emotional reactions while talking to the patient. |
4.33 |
4.32 |
0 |
194 |
1 |
| Ask personal questions of the patient cautiously. |
4.38 |
4.28 |
1.37 |
194 |
0.17 |
| Make sure the patient is comfortable. |
4.38 |
4.35 |
0.32 |
194 |
0.74 |
| Solve patient problems while maintaining emotional control. |
4.15 |
4.27 |
-1.53 |
194 |
0.12 |
| Easily view issues from the patient's perspective. |
4.17 |
4.16 |
0.15 |
194 |
0.88 |
| Read patients' emotions from their faces. |
4.20 |
4.21 |
0 |
194 |
1 |
| Accept patient's positive feedback without embarrassment. |
3.27 |
4.25 |
0.16 |
194 |
0.87 |
| Understand and empathize with the patient’s feelings. |
4.24 |
4.20 |
0.52 |
194 |
0.60 |
| Accept the patient as he/she is. |
4.30 |
4.32 |
-0.22 |
194 |
0.81 |
| Apologize to the patient if needed. |
4.31 |
4.28 |
0.09 |
194 |
0.92 |
| Try to empathize with the patient during our conversation. |
4.03 |
4.10 |
-0.71 |
194 |
0.47 |
|
Teacher-student relationship (17 items)
|
| Respect the student. |
4.43 |
4.54 |
-1.43 |
194 |
0.15 |
| Have enough patience to answer students' questions. |
4.47 |
4.55 |
-1.21 |
194 |
0.22 |
| Be punctual and notify in advance if a class is canceled. |
4.43 |
4.49 |
-0.92 |
194 |
0.35 |
| Be a trusted confidant for students. |
4.46 |
4.61 |
-1.93 |
194 |
0.05 |
| Guide students if necessary. |
4.47 |
4.61 |
-2.07 |
194 |
0.039 |
| Uphold the ethical responsibilities of the teaching profession. |
4.48 |
4.59 |
-1.56 |
194 |
0.12 |
| Aim to foster students' cognitive, skill, and moral development. |
4.44 |
4.61 |
-2.27 |
194 |
0.02 |
| Maintain current knowledge, technology, and skills for students. |
4.47 |
4.56 |
-1.07 |
194 |
0.28 |
| Aim to make students and colleagues feel valued. |
4.44 |
4.54 |
-1.34 |
194 |
0.18 |
| Have authority, sincerity, and legitimacy with students. |
4.47 |
4.55 |
-1.12 |
194 |
0.26 |
| Ensure fairness in evaluating students academically. |
4.44 |
4.55 |
-1.35 |
194 |
0.17 |
| Strive to protect privacy, promote gender safety, and support students' mental health. |
4.73 |
4.54 |
0.68 |
194 |
0.49 |
| Emphasize that everyone shares the same dignity. |
4.48 |
4.55 |
-1.08 |
194 |
0.27 |
| Provide students with study details, evaluation criteria, and meeting dates. |
4.43 |
4.57 |
-2.08 |
194 |
0.039 |
| Personally warn a student if they forget a mistake. |
4.37 |
4.47 |
-1.30 |
194 |
0.19 |
| Be cheerful when attending class. |
4.47 |
4.51 |
0.47 |
194 |
0.63 |
| Do not falsely accuse any student. |
4.52 |
4.53 |
0.06 |
194 |
0.94 |
More analysis on the data in terms of the pretest and posttest scores show significant differences, reflecting improvements in specific areas of communication skills. In the Active Listening category, while the overall scores showed a slight increase, individual items revealed mixed results. For instance, the item “Show interest in listening to the patient” improved marginally from a pretest score of 4.47 to a posttest score of 4.51, indicating a positive yet statistically insignificant change (P = 0.61). Conversely, “Let the patient finish his/her speech without interrupting” demonstrated a substantial improvement from 3.40 to 4.43 (P = 0.66), suggesting a notable enhancement in this critical aspect of active listening. However, other items, such as “Allow the patient time to think before responding,” exhibited a slight decrease from 4.39 to 4.35 (P = 0.57), highlighting areas where further training may be necessary. In the Verbal Skills domain, several items reflected significant advancements. Notably, the item “Give negative feedback at the right time” showed a marked increase from 2.95 to 3.68 (P = 0.016), indicating that participants became more adept at providing constructive criticism. Similarly, “Describe others’ behavior without judgment” improved from 3.05 to 3.75 (P = 0.019), further underscoring the effectiveness of the training. However, “Welcome the patient” exhibited a decrease from 3.16 to 4.22 (P = 0.47), suggesting inconsistent application of welcoming behaviors among participants. The Non-verbal Skills category also presented a range of outcomes. While “Strive to be respectful in conversations with the patient” increased slightly from 4.46 to 4.49 (P = 0.67), the item “Use visual aids like diagrams and written information when communicating with the patient” improved significantly from 2.89 to 4.05 (P = 0.13), indicating a greater incorporation of visual aids into practice. Nevertheless, the item “Aim for the right tone of voice when speaking to the patient” showed a decrease from 4.49 to 4.40 (P = 0.17), highlighting the need for ongoing focus on tone and delivery. Within the Patient-Centered communication skills, there were notable improvements in several areas. For example, “Ask the patient about her beliefs about problems” improved significantly from 4.22 to 4.37 (P = 0.05), indicating an increased emphasis on understanding patient perspectives. However, the item “Ask the patient about her expectations” remained stable, with scores of 4.13 in both pretest and posttest assessments (P = 1), suggesting no change in this aspect of communication (Table 3).
Table 4 represents the satisfaction levels of medical doctors regarding the clinical communication skills course assessed across various dimensions. The overall mean satisfaction score was 3.98 (SD = 0.18), indicating a generally positive response to the course. As shown in Table 4, specifically, participants reported high satisfaction with the course instructors’ expertise, achieving a mean score of 4.08 (SD = 0.28). This suggests that the medical doctors were perceived as knowledgeable and effective in delivering the course content. Additionally, the item “I recommend the clinical communication skills course to others” received a mean score of 4.17 (SD = 0.70), further emphasizing the participants’ endorsement of the course. In terms of course content, the mean satisfaction scores were also favorable. Both the length and content of the course received a mean score of 3.94 (SD = 0.23), indicating that participants found these aspects satisfactory. The organization of the course content was rated slightly lower, with a mean score of 3.80 (SD = 0.40), suggesting room for improvement in this area. Participants also expressed satisfaction with the quality of the course, reflected in a mean score of 3.82 (SD = 0.38), and their ability to establish rapport with fellow participants, which scored 3.82 (SD = 0.45). Furthermore, the course’s effectiveness in improving communication skills learning was rated at 3.80 (SD = 0.53), highlighting its perceived educational value. Finally, the item “The content of the clinical communication skills course was useful to me” achieved the highest mean score of 4.34 (SD = 0.48), indicating that participants found the material particularly applicable to their professional practice. In a similar line, medical doctors’ perceptions of the communication skills course are shown in Table 4.
Table 4.
Medical doctors’ satisfaction from the communication skill course
|
Items
|
Satisfaction
|
|
Mean
|
Standard deviation
|
| I am satisfied with the length of the clinical communication skills course. |
3.94 |
0.23 |
| I am satisfied with the contents of the clinical communication skills course. |
3.94 |
0.23 |
| I am satisfied with the organization of the contents of the clinical communication skills course. |
3.80 |
0.40 |
| I am satisfied with the quality of the clinical communication skills course. |
3.82 |
0.38 |
| I was able to establish a good rapport with the participants of the course. |
3.82 |
0.45 |
| This course improved my communication skills learning. |
3.80 |
0.53 |
| I am satisfied with the course instructors' expertise. |
4.08 |
0.28 |
| I recommend the clinical communication skills course to others. |
4.17 |
0.70 |
| The clinical communication skills course met my educational needs. |
4.08 |
0.28 |
| The content of the clinical communication skills course was useful to me. |
4.34 |
0.48 |
| Total |
3.98 |
0.18 |
|
Perception of medical doctors on communication skills course
|
Advantages and benefits:
The course enhanced my ability to communicate effectively with patients and students.
It provided valuable insights into non-verbal communication and its impact on patient interactions.
The interactive nature of the course fostered a supportive learning environment.
Role-playing scenarios helped me apply theoretical knowledge in real-life contexts.
Areas for improvement:
More case studies could provide deeper insights into complex communication challenges.
Additional focus on conflict resolution strategies would be beneficial.
Longer sessions would allow for more practice and feedback.
Relevance to work:
Effective communication is crucial in the clinical setting; this course directly applies.
The skills learned are essential for teamwork in the clinical settings.
This course made me more aware of the impact of communication on patient trust and compliance.
Impact on performance:
I feel more confident in my interactions with patients, students, and colleagues.
Since the course, I have noticed a positive change in patient feedback regarding communication.
The course has made me a more empathetic clinician, improving my interactions with the care team. |
Discussion
This study aimed to identify, design, and evaluate a communication skills course for medical doctors at Yasuj University of Medical Sciences. The findings of the present study underscore the critical importance of effective communication skills in the clinical setting, particularly among medical doctors. Similar studies have been done on residents,29 as well as nutritionists30 to assess the impact of a communication skills course, highlighting its positive effect on their communication skills. With 196 participants, including a diverse representation of medical doctors, nursing staff, and students, the present study provides valuable insights into the current state of communication skills and the impact of targeted training interventions.
The assessment of pre-test and post-test scores on communication skills revealed notable improvements, particularly in areas identified as needing enhancement. For instance, the significant increase in the ability to “Let the patient finish his/her speech without interrupting” (from 3.40 to 4.43, P = 0.66) suggests that the training effectively addressed critical components of active listening, which is essential for fostering patient-centered care.31 However, the mixed results in other areas, such as the decrease in “Allow the patient time to think before responding,” indicate that continuous training and reinforcement may be necessary to maintain and further develop these skills.32 Our research findings on the active listening items contradicts with results of the study by Makarem et al, concluding that behaviors indicating active listening rarely occur in medical doctors.33 We assume that active listening constitutes a critical component of effective communication, particularly within the medical profession, where practitioners must engage with patients to establish trust and accurately identify their primary concerns. This skill serves as the cornerstone of respectful communication and conduct, necessitating both practice and commitment rather than occurring spontaneously.
The findings regarding verbal skills are particularly noteworthy. The marked improvement in the ability to “Give negative feedback at the right time” (from 2.95 to 3.68, P = 0.016) and “Describe others’ behavior without judgment” (from 3.05 to 3.75, P = 0.019) reflect a growing awareness among medical doctors of the importance of constructive criticism in clinical settings. This aligns with literature emphasizing the role of effective feedback in enhancing team dynamics and improving patient outcomes.34 Nevertheless, the decline in welcoming behaviors suggests that while some aspects of communication have improved, others require ongoing attention.35
Furthermore, the low pre-test score of 2.89 for using visual aids highlights a significant gap in communication practices that could hinder patient understanding and engagement. The post-test score of 4.05 indicates a positive shift, yet the initial low score suggests that medical doctors may not traditionally prioritize visual aids in their communication strategies. This finding is consistent with research demonstrating that visual aids can enhance patient comprehension and retention of information.36
In a study conducted by Rezaian et al. findings revealed that the mean of communication skills was at a level needing more training in this regard.18 By the same token, research findings of Attarha et al indicates the need for on-going training in communications skills to improve teacher-student relationship in the educational process.21
The satisfaction levels reported by medical doctors regarding the clinical communication skills course were generally positive, with an overall mean score of 3.98. Participants expressed high satisfaction with the instructors’ expertise and the applicability of the course content to their professional practice. This is in line with studies that advocate for continuous professional development in communication skills, highlighting their relevance in clinical practice.32
Participants acknowledged several advantages of the course, including enhanced ability to communicate effectively with patients and the supportive learning environment fostered through interactive methods. However, they also identified areas for improvement, such as the inclusion of more case studies and a focus on conflict resolution strategies. This feedback aligns with educational theories emphasizing the importance of practical application and scenario-based learning in developing effective communication skills.37
This study has its own limitations. First, the evaluation of communication skills relied on self-reported measures and participant feedback, which may introduce bias. Participants might have overestimated their improvements due to social desirability or the Hawthorne effect. Second, as a quasi-experimental design with a one-group pretest-posttest approach, the study did not include a control group. This limits the ability to attribute observed changes in communication skills solely to the training intervention, as other external factors may have influenced the results. Third, the study did not include a long-term follow-up to assess the sustainability of the communication skills acquired during the training. Without this, it is unclear whether the benefits of the training will persist over time. The last but not least, the study was conducted at a single institution, which may limit the applicability of the findings to other contexts, healthcare settings, or educational institutions.
Implications for practice
The implications of this study extend beyond individual skill enhancement; it underscores the necessity of integrating communication training into the broader contexts for medical doctors. Effective communication is not only vital for patient satisfaction and compliance but also for fostering a collaborative team environment, which is crucial in high-stakes clinical settings like emergency departments.38 Also, the findings of this study underscore the critical need for integrating communication skills training into the medical curriculum. Given that effective communication is essential for patient care and professional interactions, medical education programs should prioritize these skills as a core component of their training. This can be achieved by developing a structured curriculum that includes both theoretical instruction and practical applications, such as role-playing and scenario-based exercises.
Future longitudinal studies should explore the long-term impact of communication skills training on healthcare professionals’ performance and patient outcomes. This could involve tracking participants over several years to evaluate whether skills acquired during training are maintained and utilized in clinical practice.
Conclusion
The significant improvements in communication skills and feedback delivery highlight the course’s success in addressing critical communication gaps. However, ongoing training is needed to enhance areas such as patient engagement and welcoming behaviors. Participants reported high satisfaction with the course’s relevance and applicability, emphasizing the importance of continuous professional development in communication skills. Overall, these findings underscore the vital role of effective communication in the clinical setting. The assessment of educational environments is a matter of consideration39-41 and the applications of mixed-methods design42 can augment the reliability of findings, thus, more researches on the topic under investigation using this methodology is recommended.
Competing Interests
The authors declare no competing interest.
Ethical Approval
This study was approved by research ethics committees of shiraz university of medical sciences with the code number: IR.SUMS.REC.1400.656. Oral informed consent was obtained from all participants.
Acknowledgements
We appreciate the Research Deputy of Shiraz University of Medical Sciences funding this research. The authors of this study also consider it necessary to thank and appreciate all participants’ efforts and sincere cooperation.
References
- Vakili MM, Hidarnia A, Niknami S, Mousavinasab SN. Effect of communication skills training on health belief model constructs about AIDS in Zanjan health volunteers (2010-11). J Adv Med Biomed Res 2011; 19(77):78-93. [ Google Scholar]
- Ahmadi MS. Effectiveness of training communication skills on self-regulated learning of male high school students in Zanjan city. Knowl Res Appl Psychol 2014;15(1):113-20. [Persian].
- Rezaei H, Bahman Bijari B, Beigzadeh A, Seyed Askari SM, Khadir E. Job satisfaction and organizational commitment of nurses in teaching hospitals affiliated to Kerman University of Medical Sciences. Iran J Med Educ 2017;17:245-50. [Persian].
- Slade D, Manidis M, McGregor J, Scheeres H, Chandler E, Stein-Parbury J, et al. Communicating in Hospital Emergency Departments. Springer; 2015.
- Olde Bekkink M, Farrell SE, Takayesu JK. Interprofessional communication in the emergency department: residents’ perceptions and implications for medical education. Int J Med Educ 2018; 9:262-70. doi: 10.5116/ijme.5bb5.c111 [Crossref] [ Google Scholar]
- Eisenberg EM, Murphy AG, Sutcliffe K, Wears R, Schenkel S, Perry S, Vanderhoef M. Communication in emergency medicine: implications for patient safety. Commun Monogr 2005; 72(4):390-413. doi: 10.1080/03637750500322602 [Crossref] [ Google Scholar]
- Seyed Askari SM, Rozbehi A, Bahman Bijari B, Mahdavinia J, Beigzadeh A, Rezaei H. Assessment of training needs of education experts in Kerman University of Medical Sciences. Am J Educ Res 2016; 4(10):736-40. doi: 10.12691/education-4-10-5 [Crossref] [ Google Scholar]
- Torabi A, Zahiri M. Study on influencing factors relationship between teacher and student in view of students of Ahvaz University of Medical Sciences. Jundishapur Sci Med J 2012;11(5):549-57. [Persian].
- Rezaee AM, Delavar A, Ahadi H, Dortaj F. Construction and validation of Iran students’ evaluation of educational quality. Quarterly of Educational Measurement 2010;1(1):1-25. [Persian].
- Yunus MM, Wan Osman WS, Mohd Ishak N. Teacher-student relationship factor affecting motivation and academic achievement in ESL classroom. Procedia Soc Behav Sci 2011; 15:2637-41. doi: 10.1016/j.sbspro.2011.04.161 [Crossref] [ Google Scholar]
- Paterson B, Crawford M. Caring in nursing education: an analysis. J Adv Nurs 1994; 19(1):164-73. doi: 10.1111/j.1365-2648.1994.tb01064.x [Crossref] [ Google Scholar]
- Akbari M, Moeintaghavi A, Ghanbari H, Bageri M, Otoufi A. A comparison of the students’ and teachers’ viewpoints about the characteristics of a good teacher in dentistry. J Mashhad Dent Sch 2014; 38(4):281-90. doi: 10.22038/jmds.2014.3148.[Persian] [Crossref] [ Google Scholar]
- Bahador H, Faraji Armaki A, Ghorbani R, Dehghani E. Effective factors on communication between teacher and student medical students of basic sciences level view. Education Strategies in Medical Sciences 2014;6(4):195-200. [Persian].
- Obeidi N. Effective factors on the communication between students and faculty members in the viewpoint of paramedical students. Education Strategies in Medical Sciences 2010;3(3):133-6. [Persian].
- Hasani L, Aghamolaie D. Communication barriers between nurses and elderly patients. J Hormozgan Univ Med Sci 2010;14(4):312-8. [Persian].
- Choi K, Lee D, Olson DL. Service quality and productivity in the US airline industry: a service quality-adjusted DEA model. Serv Bus 2015; 9(1):137-60. doi: 10.1007/s11628-013-0221-y [Crossref] [ Google Scholar]
- Managheb SE, Jaafarian J, Firouzi H. The impact of communication skills training based on Calgary- Cambridge guideline on knowledge, attitude and practice of family physicians in Jahrom University of Medical Sciences 2007. Pars J Med Sci 2022; 6(3):74-84. doi: 10.29252/jmj.6.3.4.74.[Persian] [Crossref] [ Google Scholar]
- Rezaeian M, Zare-Bidaki M, Bakhtar M, Kargar S. A survey on communication skills of Rafsanjan University of Medical Sciences Faculty Members in 2013. J Rafsanjan Univ Med Sci 2015;14(5):417-26. [Persian].
- Yazdani E, Soleimanpour Omran M. the relationship between communication skills and quality of teaching in university lecturers from the viewpoint of medical students. J North Khorasan Univ Med Sci 2018; 9(4):83-90. doi: 10.29252/nkjmd-090412.[Persian] [Crossref] [ Google Scholar]
- Soltani Arabshahi SK, Ajami A, Siabani S. Investigation of doctor-patient communication skills teaching: medical learners’ perception (Stager-Intern) and staffs of Iran University of Medical Sciences & Kermanshah University of Medical Sciences. Razi J Med Sci 2004;11(41):423-31. [Persian].
- Attarha M, Shamsi M, Akbari Torkestani N. Faculty members’ communication skills in educational process in Arak University of Medical Sciences. Iran J Med Educ 2012;12(9):676-85. [Persian].
- Zamani A, Shams B, Farajzadegan Z, Tabaeian SM. The viewpoints of clinical faculty members about teaching communication skills to medical students. Iran J Med Educ 2003;3(1):44-9. [Persian].
- Tavakol M, Murphy R, Torabi S. A needs assessment for a communication skills curriculum in Iran. Teach Learn Med 2005; 17(1):36-41. doi: 10.1207/s15328015tlm1701_7 [Crossref] [ Google Scholar]
- Chan TM, Wallner C, Swoboda TK, Leone KA, Kessler C. Assessing interpersonal and communication skills in emergency medicine. Acad Emerg Med 2012; 19(12):1390-402. doi: 10.1111/acem.12030 [Crossref] [ Google Scholar]
- Grudzen CR, Emlet LL, Kuntz J, Shreves A, Zimny E, Gang M. EM Talk: communication skills training for emergency medicine patients with serious illness. BMJ Support Palliat Care 2016; 6(2):219-24. doi: 10.1136/bmjspcare-2015-000993 [Crossref] [ Google Scholar]
- Moreira ME, French AJ. Communication in Emergency Medicine. Oxford University Press; 2019.
- Smidt A, Balandin S, Sigafoos J, Reed VA. The Kirkpatrick model: a useful tool for evaluating training outcomes. J Intellect Dev Disabil 2009; 34(3):266-74. doi: 10.1080/13668250903093125 [Crossref] [ Google Scholar]
- McKenna L, Brooks I, Vanderheide R. Graduate entry nurses’ initial perspectives on nursing: content analysis of open-ended survey questions. Nurse Educ Today 2017; 49:22-6. doi: 10.1016/j.nedt.2016.11.004 [Crossref] [ Google Scholar]
- Barbosa M, Del Piccolo L, Barbosa A. Effectiveness of a brief training program in relational/communication skills for medical residents. Patient Educ Couns 2019; 102(6):1104-10. doi: 10.1016/j.pec.2019.01.013 [Crossref] [ Google Scholar]
- Notaras S, Mak M, Wilson N. Advancing practice in dietitians’ communication and nutrition counselling skills: a workplace education program. J Hum Nutr Diet 2018; 31(6):725-33. doi: 10.1111/jhn.12569 [Crossref] [ Google Scholar]
- McCabe C. Nurse-patient communication: an exploration of patients’ experiences. J Clin Nurs 2004; 13(1):41-9. doi: 10.1111/j.1365-2702.2004.00817.x [Crossref] [ Google Scholar]
- Kurtz S, Draper J, Silverman J. Teaching and Learning Communication Skills in Medicine. CRC Press; 2017.
- Makarem A, Movaffaghi Z, Hosseini FS, Beiraghi N, Heshmati Nabavi F, Khaje Daluee M. Clinical medical teachers’ competency of active listening in Mashhad University of Medical Sciences. Iran J Med Educ 2013;12(12):935-46. [Persian].
- Hattie J, Timperley H. The power of feedback. Rev Educ Res 2007; 77(1):81-112. doi: 10.3102/003465430298487 [Crossref] [ Google Scholar]
- Lambert BL, Street RL, Cegala DJ, Smith DH, Kurtz S, Schofield T. Provider-patient communication, patient-centered care, and the mangle of practice. Health Commun 1997; 9(1):27-43. doi: 10.1207/s15327027hc0901_3 [Crossref] [ Google Scholar]
- Garcia-Retamero R, Cokely ET. Designing visual aids that promote risk literacy: a systematic review of health research and evidence-based design heuristics. Hum Factors 2017; 59(4):582-627. doi: 10.1177/0018720817690634 [Crossref] [ Google Scholar]
- Kolb DA. Experiential Learning: Experience as the Source of Learning and Development. FT Press; 2014.
- Roh H, Park KH. A scoping review: communication between emergency physicians and patients in the emergency department. J Emerg Med 2016; 50(5):734-43. doi: 10.1016/j.jemermed.2015.11.002 [Crossref] [ Google Scholar]
- Beigzadeh A, Naghibzadeh Tahami A, Rezaei H, Bahman Bijari B, Nazarieh M, Seyed Askari SM. Epidemiology of trauma in Shahid Bahonar hospital in Kerman. J Emerg Pract Trauma 2016; 2(2):33-6. doi: 10.15171/jept.2015.16 [Crossref] [ Google Scholar]
- Salajegheh M, Bahman Bijari B, Shokouhi M, Safipour Afshar A, Beigzadeh A. Educational environment assessment at outpatient clinics in teaching hospitals of Kerman University of Medical Sciences, Iran, from resident’s perspective based on the ACLEEM questionnaire. Stride Dev Med Educ 2015;12(Suppl):119-30. [Persian].
- Beigzadeh A, Yamani N, Bahaadinbeigy K, Adibi P. Challenges and strategies of clinical rounds from the perspective of medical students: a qualitative research. J Educ Health Promot 2021; 10:6. doi: 10.4103/jehp.jehp_104_20 [Crossref] [ Google Scholar]
- Bazrafshan A, Haghdoost A, Rezaie H, Beigzadeh A. A practical framework for evaluating health services management educational program: the application of the mixed-method sequential explanatory design. Res Dev Med Educ 2015; 4(1):47-54. doi: 10.15171/rdme.2015.008 [Crossref] [ Google Scholar]