Res Dev Med Educ. 14 :33294.
doi: 10.34172/rdme.025.33294
Original Article
The effect of ASLS instruction on the knowledge and skills of medical students in Tabriz University of Medical Sciences, Iran, Single group pre-and post-test design
Alireza Ala Data curation, Methodology, Project administration, Resources, Supervision, Writing – review & editing, 1 
Samad Shams Vahdati Conceptualization, Investigation, Project administration, Resources, Supervision, Writing – review & editing, 1
Parya Tahmasebi Conceptualization, Investigation, Writing – review & editing, 1
Neda Gilani Writing – original draft, Writing – review & editing, 1
Amin Abbasi Writing – original draft, Writing – review & editing, 2
Reza Aletaha Methodology, Software, Writing – review & editing, 3, *
Author information:
1Emergency and Trauma Care Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
2Endocrine Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
3Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Background:
Given the higher burden of stroke in Iran compared to many high-income countries, this study aimed to investigate the effect of Advanced Stroke Life Support (ASLS) training on enhancing the prehospital performance of medical caregivers in Tabriz, Iran.
Methods:
Medical interns at Tabriz University of Medical Sciences participated in an ASLS training course consisting of lectures and group sessions that consisted of video-based case education on stroke diagnosis and management, alongside hands-on training in using standardized stroke assessment tools (CPSS, MEND, NIHSS) for simulated patients. Participants’ performance in stroke knowledge and management was assessed using a test exam before and after the ASLS course, and their scores were compared.
Results:
The results showed that participants scored 61.30% and 84.13% before and after the ASLS course, respectively, indicating a significant improvement (P=0.001). However, their improvement was not the same in different stroke education fields, such as epidemiology, etiology, diagnosis, and management.
Conclusion:
Our study demonstrated that the ASLS course can be used as an effective way to improve skills and knowledge in managing stroke patients.
Keywords: Caregivers, Education, Emergency medical services, Stroke
Copyright and License Information
© 2025 The Author(s).
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, as long as the original authors and source are cited. No permission is required from the authors or the publishers.
Funding Statement
None.
Introduction
The World Health Organization (WHO) defined stroke in 1970, characterizing it as the rapid onset of clinical symptoms, indicating a localized or widespread disruption of cerebral function. These symptoms must persist for more than 24 hours or result in death, and there should be no identifiable cause other than vascular origin.1
One in 20 deaths in the US is caused by stroke, accounting for approximately 140,000 deaths annually in the nation. As a result, this condition ranks as the fifth most prevalent cause of mortality in the United States. Furthermore, in the US, it is the main factor contributing to long-term disability.2 Moreover, according to a study conducted in 2017, the financial burden of stroke was estimated to be €45 billion. This estimate encompasses both the direct costs of providing care and the indirect costs associated with productivity loss.3 The prevalence of stroke is steadily rising throughout the Middle East and North Africa (MENA) region, and it is predicted that by 2030, the current mortality rate will double.4 Furthermore, the importance of stroke management studies in Iran cannot be overstated, particularly given the high prevalence of stroke as a leading cause of disability and mortality within the country, which is higher than most Western countries.5 Moreover, studies conducted by Kazemi et al emphasize the need for specialized stroke care units and trained personnel, as inadequacies in these areas profoundly influence in-hospital mortality rates among stroke patients.6
Multiple difficulties are presented by the massive and ever-growing burden of stroke. Despite bearing the majority of the burden, low- and middle-income countries (LMICs) only receive a tiny portion of the world’s financial and medical resources.7 Additionally, strokes strike people in LMICs approximately 15 years sooner than they do in high-income countries (HICs), which has a significant detrimental effect on socioeconomic growth since these people are most impacted while they are at the height of their productive lives.8,9
With the ongoing growth of populations and the increasing lifespan of individuals, it is anticipated that there will be a significant rise in the occurrence of stroke events and their subsequent long-term consequences. That is why the associated financial burden is also expected to escalate.10
Prehospital responders who have received specialized training in promptly evaluating and identifying the indicators and manifestations of stroke possess the ability to promptly notify a suitably equipped and adequately staffed medical facility, thereby ensuring preparedness to validate the initial diagnosis and promptly initiate the appropriate therapeutic interventions.
For this reason, Advanced Stroke Life Support® (ASLS®) is designed for prehospital personnel on the scene, emergency department nurses and physicians, and along the continuum of care to the stroke or critical care unit. Currently, there is not enough evidence examining the effect of ASLS instruction. However, a prior study investigated practicing healthcare professionals in high-resource settings. Our study uniquely targets medical interns in a high-burden LMIC context, directly addressing urgent training needs and resource limitations in stroke care.11 To raise the standard of diagnostic and therapeutic services and to advance the profession generally, the current research will examine the effects of teaching medical students the ASLS curriculum on their knowledge and clinical skills.
Methods
Study Design
This study is Single group pre- and post-test design at an academic medical center in Tabriz University of Medical Sciences, Iran.
Setting
This study was conducted at an academic medical center in Tabriz University of Medical Sciences, Iran.
Participants
The participants were medical interns at the time of study conduct. Internship is the final 1.5 years of the medical school program in which students are involved practically at the patient’s bedside. All interns of Tabriz University of Medical Science were included in the study
except for those who were guest students, unwilling to participate, did not answer the first and/or second exam, or did not participate in classes attended for ASLS learning.
Interventions
All participants were engaged in a one-day evidence-based workshop for ASLS learning taught by certified instructors from approved centers who had completed the comprehensive ASLS teaching course. All instructors underwent formal ASLS instructor training and certification before the course. Furthermore, we confirm that the course content and delivery adhered strictly to international ASLS standards, ensuring consistency and quality in the educational intervention.
The workshop included 3.5 hours of educational lectures covering core topics such as epidemiology, pathophysiology, anatomy, signs and symptoms of stroke, and management of related syndromes. This was followed by 4.5 hours of interactive group sessions designed to promote application of knowledge in realistic clinical scenarios. During the group sessions, participants—divided into small groups and guided by trained facilitators—reviewed and discussed clinical scenarios presented through educational videos, which simulated patients with symptoms of acute stroke or stroke mimics. These sessions also included hands-on training with standardized assessment tools such as the Cincinnati Prehospital Stroke Scale (CPSS), the Miami Emergency Neurologic Deficit (MEND), and the National Institutes of Health Stroke Scale (NIHSS), enabling participants to practice conducting neurological assessments and planning appropriate diagnostic and treatment strategies for simulated stroke cases under instructor supervision. Facilitators actively encouraged critical thinking, collaboration, and reflective discussion to reinforce key concepts and foster the integration of theoretical knowledge with practical clinical skills.
The participants were tested by an exam in 5 different major fields of stroke syndrome, MEND basic test score, review of treatment options, and posthospitalization care before the start of the course, and then they participated in the ASLS course. After completing the course, the same test was repeated to assess the knowledge and skills of medical interns in the management of stroke before and after participating in the ASLS course. Hard questions in tests referred to items in the assessment that required the application of complex clinical reasoning or integration of multiple ASLS concepts, rather than simple recall of facts, and fewer than 50 interns were able to answer correctly in the pre-test and post-test. These questions are important because they better reflect real-world decision-making challenges and allow us to more accurately evaluate higher-order learning outcomes resulting from the training. Furthermore, the test items were reviewed by a panel of stroke and medical education experts to ensure content validity.
Outcomes
Assessing the knowledge and skills of medical interns in the management of stroke before and after attending ASLS course.
Statistical Methods
Descriptive statistics (mean ± standard deviation) were used to report the results of the study. The normality of the data was checked using the Kolmogorov‒Smirnov test, and since the data distribution was normal, a paired t test was used to compare the average score of the test before and after completing the course. A P value of 0.05 or less was considered statistically significant. All analyses were performed using SPSS software version 25.
Results
Participants
A total of 105 medical interns participated in the study and completed the pre-test, ASLS course, and post-test. There was no drop off of the study.
Main Results
Among all 6 major fields of pre-test, stroke epidemiology was the one interns chose the correct answer (78.6%), while more than half of the interns failed to answer the stroke etiology questions (46.5%). Table 1 demonstrates the percentage of correct answers in each field in the pre-test.
Table 1.
pre-test, post-test, and progress of scores after attending ASLS course
|
Fields
|
Pre-test
|
Post-test
|
Progress (%)
|
|
Number of questions
|
Correct answers (%)
|
Number of questions
|
Correct answers (%)
|
| Stroke epidemiology |
2 |
78.6 |
2 |
96.2 |
17.6 |
| Stroke etiology |
5 |
46.5 |
4 |
82.4 |
35.9 |
| Stroke symptoms |
3 |
56.2 |
4 |
70.0 |
13.8 |
| Diagnosis and differential diagnosis of stroke |
4 |
64.8 |
3 |
95.5 |
30.7 |
| Management and treatment of stroke |
4 |
73.6 |
5 |
95.5 |
21.9 |
| administration of thrombolytics |
2 |
48.1 |
2 |
65.2 |
17.1 |
After attending the ASLS course, most of the interns answered correctly to the post-test questions in the fields of stroke epidemiology (96.2%), diagnosis and differential diagnosis of stroke (95.5%), and management and treatment of stroke (95.5%). The field of administration of thrombolytics was the one with the lowest correct answer rate among other fields (65.2%). (Table 1).
Interns had the most progress in the fields of stroke etiology, diagnosis and differential diagnosis of stroke, and management and treatment of stroke, with percentages of 35.9%, 30.7%, and 21.9%, respectively (Table 1).
The mean scores of interns in the pre-test and post-test were 12.95 and 17.06 out of 20, respectively. The distribution of scores in the pre-test and post-test is shown in Figure 1.
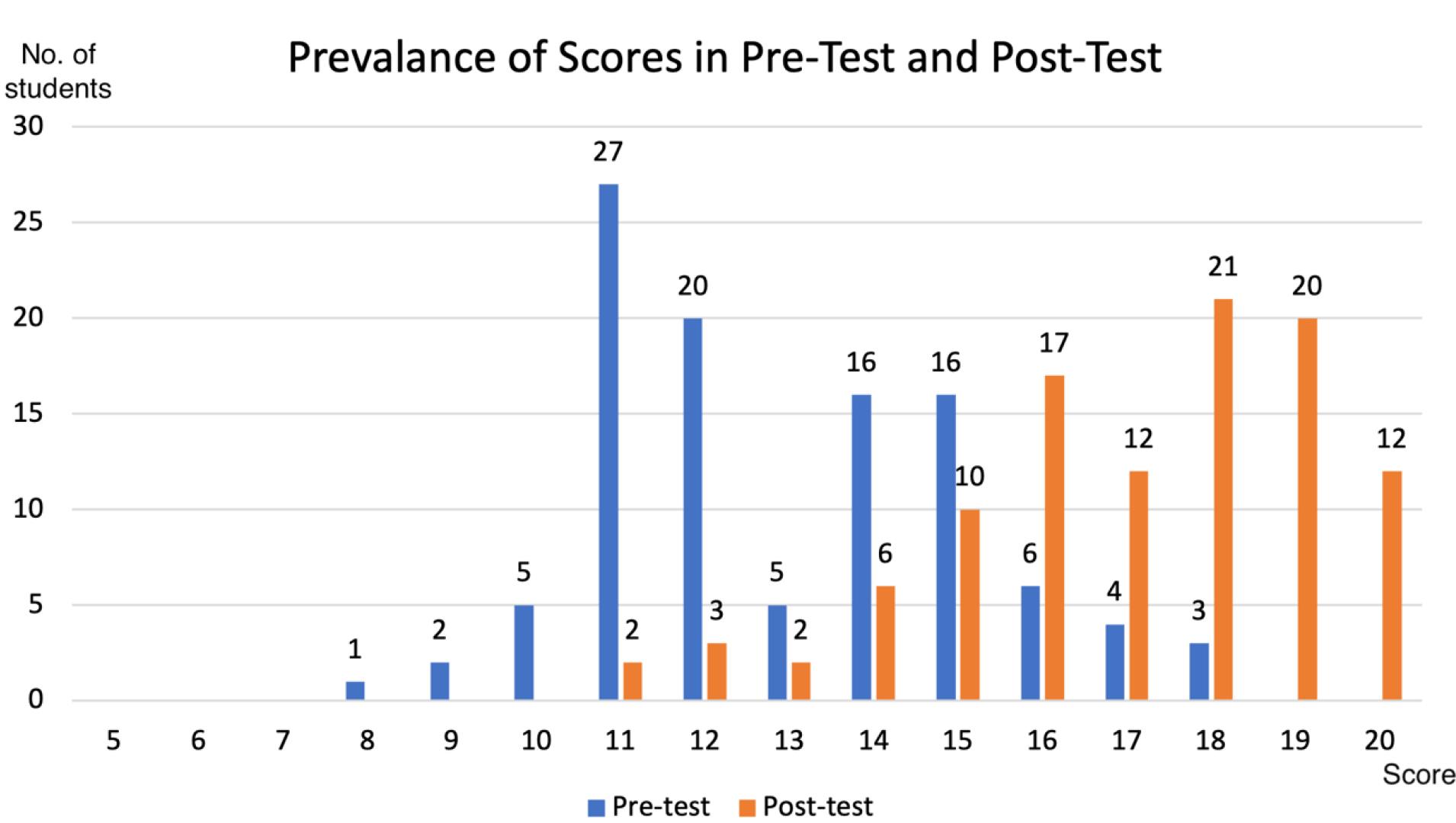
Figure 1.
Prevalence of scores in pre-test and post-test
.
Prevalence of scores in pre-test and post-test
There were 4 hard questions among all 20 questions of the exam. Hard questions were assumed to be those that fewer than 50 interns were able to answer correctly in the pre-test and post-test.
When comparing the scores before (61.30%) and after (84.13%) the ASLS course, there was a statistically significant difference between them, with a P value of 0.001.
In the knowledge fields, including stroke epidemiology, stroke etiology, stroke symptoms, and diagnosis and differential diagnosis of stroke, there was a statistically significant improvement when comparing pre-test (53.61%) and post-test (80.03%) scores (P value = 0.019).
In contrast with knowledge fields, the differences between skill fields, including management and treatment of stroke and administration of thrombolytics, in the pre-test (60.85%) and post-test (80.35%) were not statistically significant (P value = 0.078).
Discussion
The present study is the first ASLS evaluation in Iranian medical interns, highlighting challenges in thrombolytic training. This study included 105 medical students from the Tabriz University of Medical Sciences. After ASLS training, students showed improvement in knowledge and skills related to stroke management, including epidemiology, diagnosis, and treatment. The greatest improvements were observed in the causes, diagnosis, and management of stroke. A comparison of the results before and after training showed that 61.30% of the answers were correct before the training, whereas 84.13% of the answers were correct in the post-test, indicating a significant difference. Similarly, another study showed the effect of a stroke education program on students’ and parents’ performance on a stroke questionnaire. The correct test scores for students before, within one week, and three months after stroke education were 54.49% versus 55.03% (P = 0.418), 98.69% versus 60.89% (P < 0.001), and 95.58% versus 75.7% (P < 0.001) in the intervention and control groups, respectively. The correct test scores for parents at the same time points were 68.78% versus 64.47% (P = 0.107), 96.89% versus 71.42% (P < 0.001), and 94.58% versus 76.54% (P < 0.001) in the intervention and control groups, respectively.12
Our study demonstrated that in terms of knowledge (epidemiology of stroke, causes of stroke, stroke symptoms, and differential diagnosis and complications of stroke), 53.61% of the answers were correct in the pre-test, and 86.03% were correct in the post-test, showing a statistically significant difference. Similarly, Anzardo et al reported a significant increase in knowledge and awareness among hospital and prehospital service providers before and after ASLS training. The average level of awareness before training was 64.4%, which increased to 89.1% after the training.11 The study by Jones and Campbell also found a significant difference in participants’ level of awareness before and after ASLS training. Before the training, 47 out of the 50 participants received an unacceptable score ranging from 35 to 85 on the test. After completing the course, all the participants scored between 80 and 100 points.13 Our study also reported that in terms of skills (management and treatment of stroke and thrombolytic injection techniques), 60.85% of the answers were correct in the pre-test and 80.35% were correct in the post-test; however, the difference was not statistically significant. Non-significant gains observed in skill domains such as thrombolytics could be due to lack of sufficient hands-on training; these complex clinical skills typically require more time and repeated practical experience to show significant improvement, something that may not be achievable through brief or primarily theoretical sessions. Furthermore, the lack of skill retention observed in the study likely reflects gaps in the curriculum; specifically, insufficient simulation time and limited opportunities for repeated practice, both of which are essential for consolidating and maintaining complex clinical skills over time. Moreover, LMIC-specific barriers, including limited access to simulation equipment, fewer trained instructors, high trainee workloads, and constrained time and space for hands-on learning, can significantly challenge ASLS implementation. These resource constraints may reduce the effectiveness or scalability of the curriculum, highlighting the need for locally adapted approaches if ASLS is to be successfully implemented in similar settings elsewhere.
Previous studies have shown the effect of ASLS training on the prehospital management of stroke patients and their early referral to the hospital. A study by Henry-Morrow in 2017 demonstrated that ASLS training for EMS providers led to an increase in the number of stroke patients calling for emergency services as a prehospital center.14 Alberts et al showed a significant association between early referral of stroke patients to hospitals and prior stroke educational programs. The rate of reference to the hospital within 24 hours of symptom onset was 37% in patients without education compared with 86% in patients who received education.15 A study by Mullen Conley et al demonstrated the effectiveness of an educational stroke program for students. Students who received education were better at identifying stroke symptoms and calling 911 upon witnessing a stroke.16 In another study, studies regarding factors associated with the prehospitalization time of stroke patients were reviewed, and no relationship was demonstrated between stroke knowledge and prehospital delay, in contrast to the studies mentioned above.17
There have been studies that showed the effect of comprehensive stroke education on improving stroke knowledge, similar to the ASLS training in our study. A study by Stern et al demonstrated that the discussion and involvement of participants in a stroke education program were necessary to achieve acceptable results in improving stroke knowledge.18 Yang et al showed the effectiveness of a comprehensive stroke education program compared with conventional oral education. Subjects who received comprehensive education had significantly better prehospital delays and presymptomatic stroke alert tests.19 Amano et al used facial droop, arm weakness, speech disturbance, and time to call an ambulance (FAST) mnemonic as a means for stroke education programs in their study. It was demonstrated that students and parents who participated in the FAST stroke education program performed significantly better in answering the stroke knowledge questions.20 So, to increase the feasibility and impact of ASLS in low-resource settings, we recommend adaptations such as integrating simplified stroke recognition tools like the FAST mnemonic. These modifications help address resource limitations while still reinforcing core clinical competencies. Furthermore, recent innovations in stroke education have increasingly leveraged technology to address traditional training gaps.21 Moreover, gamification approaches have also shown promise for reinforcing rapid stroke recognition and decision-making, leading to better knowledge retention and improved motivation among trainees.22-25 These advancements suggest that integrating immersive and interactive methods, alongside classic ASLS content, could further strengthen stroke training effectiveness.
Limitations
The present study has some limitations. First, this study only tested students’ performance on a stroke questionnaire and could not evaluate their performance in a stroke emergency in the field. Second, there were no further evaluations to see if students lost their knowledge and skills over time; therefore, follow-up evaluations would be useful. There is a clear need for longitudinal studies to assess skill retention after ASLS training, as short-term evaluations may miss whether practical competencies are sustained over time, especially in resource-limited settings where ongoing reinforcement and follow-up are crucial for lasting impact. Third, the participants in our study were medical students, and considering their prior knowledge of stroke, our results may not apply to the general population. Carrying out this study on the general population with general prior medical knowledge is recommended. Fourth, no pilot testing was performed, which may reduce the reliability of the tests. For increasing the reliability of tests, future studies should include pilot testing with a group of medical students not participating in the main study. Fifth, the single-group pre- and post-test design may inflate the apparent efficacy of the intervention, as it lacks a control group to account for factors like maturation bias or external influences, so observed improvements cannot be confidently attributed to the ASLS training alone. Future research using controlled or randomized designs is warranted to more accurately assess the impact of ASLS training. Lastly, a potential limitation of this study is the risk of recall bias or learning effects associated with administering the same test before and after the intervention, which could not be fully eliminated due to the absence of alternate test forms; however, the use of complex, application-based questions and an adequate time interval between tests were intended to help mitigate this effect.
Conclusion
Comprehensive stroke education programs are effective in increasing stroke management skills and knowledge. This study demonstrated that the ASLS training course can significantly increase participants’ scores on a stroke test exam. It was also demonstrated that the mentioned improvement was not the same in different fields of stroke knowledge, such as the administration of thrombolytics, which had the lowest correct answer rate, even after the course. The key takeaway for educators is clear: ASLS training should explicitly prioritize practical thrombolytic administration drills and other hands-on skill stations, as these areas require repeated, focused practice to achieve and sustain competency.
Competing Interests
The authors declare no conflict of interest.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
This study was approved by the ethics committee of the Tabriz University of Medical Sciences (IR.TBZMED.REC.1399.419), and all information was kept confidential. Informed consent was obtained from the participants, and all participants were free to leave the study at any time.
Acknowledgements
Special thanks to all medical students who participated in our study. This manuscript was drawn from the medical degree thesis for Dr. Parya Tahmasebi with no.: 65299.
References
- Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T. Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ 1980; 58(1):113-30. [ Google Scholar]
- Centers for Disease Control and Prevention (CDC). Stroke Facts. 2017. Available from: https://www.cdc.gov/stroke/facts.htm.
- Wilkins E, Wilson L, Wickramasinghe K, Bhatnagar P, Leal J, Luengo-Fernandez R, et al. European Cardiovascular Disease Statistics 2017. Brussels: European Heart Network; 2017.
- Azarpazhooh MR, Etemadi MM, Donnan GA, Mokhber N, Majdi MR, Ghayour-Mobarhan M. Excessive incidence of stroke in Iran: evidence from the Mashhad Stroke Incidence Study (MSIS), a population-based study of stroke in the Middle East. Stroke 2010; 41(1):e3-10. doi: 10.1161/strokeaha.109.559708 [Crossref] [ Google Scholar]
- Ghandehari K. Epidemiology of stroke in Iran. Galen Med J 2016; 5:e588. doi: 10.31661/gmj.v5i.588 [Crossref] [ Google Scholar]
- Kazemi Z, Emamgholipour Sefiddashti S, Daroudi R, Ghorbani A, Yunesian M, Hassanvand MS. Estimation and predictors of direct hospitalisation expenses and in-hospital mortality for patients who had a stroke in a low-middle income country: evidence from a nationwide cross-sectional study in Iranian hospitals. BMJ Open 2022; 12(12):e067573. doi: 10.1136/bmjopen-2022-067573 [Crossref] [ Google Scholar]
- Sliwa K, Yacoub M. Catalysing the response to NCDI Poverty at a time of COVID-19. Lancet 2020; 396(10256):941-3. doi: 10.1016/s0140-6736(20)31911-5 [Crossref] [ Google Scholar]
- Sposato LA, Saposnik G. Gross domestic product and health expenditure associated with incidence, 30-day fatality, and age at stroke onset: a systematic review. Stroke 2012; 43(1):170-7. doi: 10.1161/strokeaha.111.632158 [Crossref] [ Google Scholar]
- Bayona H, Owolabi M, Feng W, Olowoyo P, Yaria J, Akinyemi R. A systematic comparison of key features of ischemic stroke prevention guidelines in low- and middle-income vs high-income countries. J Neurol Sci 2017; 375:360-6. doi: 10.1016/j.jns.2017.02.040 [Crossref] [ Google Scholar]
- Bennett DA, Krishnamurthi RV, Barker-Collo S, Forouzanfar MH, Naghavi M, Connor M. The global burden of ischemic stroke: findings of the GBD 2010 study. Glob Heart 2014; 9(1):107-12. doi: 10.1016/j.gheart.2014.01.001 [Crossref] [ Google Scholar]
- Anzardo EV, Motola I, Brotons AA, Carter SP, Rodriguez RD, Issenberg SB. Advanced Stroke Life Support® course significantly improves knowledge of stroke diagnosis and management for prehospital and hospital-based providers. Stroke 2018; 49(Suppl 1):ATP356. doi: 10.1161/str.49.suppl_1.TP356 [Crossref] [ Google Scholar]
- Marto JP, Borbinha C, Filipe R, Calado S, Viana-Baptista M. Impact of stroke education on middle school students and their parents: a cluster randomized trial. Int J Stroke 2017; 12(4):401-11. doi: 10.1177/1747493016677980 [Crossref] [ Google Scholar]
- Jones A, Campbell G. Advanced Stroke Life Support®: making a difference in stroke care. Stroke 2015; 46(Suppl 1):AWP364. doi: 10.1161/str.46.suppl_1.wp364 [Crossref] [ Google Scholar]
- Henry-Morrow TK, Nelson BD, Conahan E, Mathiesen C, Glenn-Porter B, Niehaus MT. An educational intervention allows for greater prehospital recognition of acute stroke. Am J Emerg Med 2017; 35(12):1959-61. doi: 10.1016/j.ajem.2017.05.036 [Crossref] [ Google Scholar]
- Alberts MJ, Perry A, Dawson DV, Bertels C. Effects of public and professional education on reducing the delay in presentation and referral of stroke patients. Stroke 1992; 23(3):352-6. doi: 10.1161/01.str.23.3.352 [Crossref] [ Google Scholar]
- Mullen Conley K, Juhl Majersik J, Gonzales NR, Maddox KE, Pary JK, Brown DL. Kids Identifying and Defeating Stroke (KIDS): development and implementation of a multiethnic health education intervention to increase stroke awareness among middle school students and their parents. Health Promot Pract 2010; 11(1):95-103. doi: 10.1177/1524839907309867 [Crossref] [ Google Scholar]
- Teuschl Y, Brainin M. Stroke education: discrepancies among factors influencing prehospital delay and stroke knowledge. Int J Stroke 2010; 5(3):187-208. doi: 10.1111/j.1747-4949.2010.00428.x [Crossref] [ Google Scholar]
- Stern EB, Berman M, Thomas JJ, Klassen AC. Community education for stroke awareness: An efficacy study. Stroke 1999; 30(4):720-3. doi: 10.1161/01.str.30.4.720 [Crossref] [ Google Scholar]
- Yang L, Zhao Q, Zhu X, Shen X, Zhu Y, Yang L. Effect of a comprehensive health education program on pre-hospital delay intentions in high-risk stroke population and caregivers. Qual Life Res 2017; 26(8):2153-60. doi: 10.1007/s11136-017-1550-4 [Crossref] [ Google Scholar]
- Amano T, Yokota C, Sakamoto Y, Shigehatake Y, Inoue Y, Ishigami A. Stroke education program of act FAST for junior high school students and their parents. J Stroke Cerebrovasc Dis 2014; 23(5):1040-5. doi: 10.1016/j.jstrokecerebrovasdis.2013.08.021 [Crossref] [ Google Scholar]
- Zafar Z, Umair M, Faheem F, Bhatti D, Kalia JS. Medical education 40: a neurology perspective. Cureus 2022; 14(11):e31668. doi: 10.7759/cureus.31668 [Crossref] [ Google Scholar]
- Brown CL, Comunale MA, Wigdahl B, Urdaneta-Hartmann S. Current climate for digital game-based learning of science in further and higher education. FEMS Microbiol Lett 2018;365(21). doi: 10.1093/femsle/fny237
- Li MC, Tsai CC. Game-based learning in science education: a review of relevant research. J Sci Educ Technol 2013; 22(6):877-98. doi: 10.1007/s10956-013-9436-x [Crossref] [ Google Scholar]
- Weaver K, Roche CC. Learning the cranial nerves: a low-tech gamified teaching strategy. J Nurs Educ 2019; 58(9):553. doi: 10.3928/01484834-20190819-12 [Crossref] [ Google Scholar]
- Telner D, Bujas-Bobanovic M, Chan D, Chester B, Marlow B, Meuser J. Game-based versus traditional case-based learning: comparing effectiveness in stroke continuing medical education. Can Fam Physician 2010; 56(9):e345-51. [ Google Scholar]