Res Dev Med Educ. 14:33301.
doi: 10.34172/rdme.025.33301
Original Article
Gender discrimination in medical education: A qualitative study on structural barriers for women
Narges Bashirivand Conceptualization, Data curation, Investigation, Methodology, Resources, Software, Writing – original draft, Writing – review & editing, 1 
Fatemeh Javaheri Conceptualization, Investigation, Methodology, Project administration, Software, Supervision, Writing – original draft, 1, *
Mahasti Alizadeh Conceptualization, Methodology, Project administration, Resources, Supervision, Writing – original draft, 2
Author information:
1Department of Sociology, Faculty of Literature and Humanities, Kharazmi University, Tehran, Iran
2Medical Education Research Center, Health Management and Safety Promotion Research Institute, Department of Community Medicine, Faculty Medicine Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Background:
There is substantial theoretical and empirical evidence indicating the presence of gender discrimination in the field of medicine. By entering the medical profession, women have transcended traditional gender roles and actively engaged in professional activism, yet they continue to face structural barriers. This study aims to identify the structural aspects of gender discrimination experienced by female students in medical education, focusing on the causal, contextual, and mediating factors and their consequences.
Methods:
This qualitative study, conducted within a critical paradigm, employed grounded theory to describe and analyze the findings. The primary motivation for choosing it is to access knowledge grounded in real and up-to-date data. By fostering a deeper understanding, it serves as a reliable guide for action. The research was conducted at a University within Iran’s medical sciences. Data were collected through semi-structured interviews with fifteen, sixth- and seventh-year general medicine students.
Results:
The central category "Struggle between agency and discrimination" was identified. Key causal conditions include "gender stereotypes" and "structural discriminations". The consequences are: Suppression of capabilities & self-efficacy, psychological & mental stress, low professional advancement, sexual and psychological harm, academic exhaustion, tendency to migrate.
Conclusion:
This research offers a deeper understanding of the structural aspects of gender discrimination in medical education. By addressing specific issues within the field, it provides practical suggestions for improving conditions and reforming the medical education system to eliminate gender discrimination, drawing on sociological knowledge and a critical approach.
Keywords: Gender discrimination, Medical education, Qualitative research, Sociological study
Copyright and License Information
© 2025 The Author(s).
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, as long as the original authors and source are cited. No permission is required from the authors or the publishers.
Funding Statement
Not applicable.
Introduction
Historically, universities and medicine were male-dominated until about a century ago. Predominantly led by men, these institutions have perpetuated and reinforced norms associated with masculinity, consistently viewing men as the standard.1 While the participation and role of women in medicine today are undeniable, gender-discriminatory norms and structures persist, leading to significant inequalities in women’s medical careers.2 Gender discrimination in education, counseling, employment, career advancement, and compensation remains prevalent. The increase in the number of women in medical education, contrasted with a decline in their presence in higher education, underscores structural reasons and inconsistencies that align with gender patterns.3
To comprehend the structural dimension of gender discrimination, it is essential to consider external factors such as social structures, laws and regulations, differential rewards for men and women, and the distribution of power and positions between genders.4 The structural dimension of gender discrimination involves systemic barriers that hinder women’s professional advancement, including the scarcity of same-sex mentors and the persistence of gender-based structures in the medical field.5 This phenomenon in medical schools can result in unequal distribution of opportunities and resources between men and women. Gender inequalities in the distribution of power across occupational and institutional contexts underpin the gender division of labor and the persistence of patriarchy.6 Various types of gender discrimination are frequently experienced by medical students,7-11 eading to adverse psychological effects such as increased depression, anxiety, and academic burnout. Overt bias also significantly influences the career trajectories of students who face gender inequality, discrimination, and harassment.12,13
Gender discrimination in educational and professional environments significantly contributes to sexual misconduct against women, with sexual harassment being a prominent example. Women physicians frequently face various forms of implicit discrimination and harassment, which not only differentiate their career paths from their male counterparts but also impose physical and psychological stress, potentially affecting their sense of self-efficacy.14 In recent years, concerns about sexual assault and harassment have gained considerable attention in research, policymaking, and public discourse.15 Report numerous cases of sexual harassment and assault among female academics.16,17
Over the past three decades, Iran has experienced a significant increase in women entering the field of medicine, mirroring trends observed in other societies. Since the mid-1990s, the number of female entrants has surged dramatically. Over a decade, the number of women admitted to the medical field increased four and a half times compared to a decade ago, while the number of men increased one and a half times. During this period, approximately 70% of medical entrants were women and 30% were men. However, studies indicate that despite the high number of women entering medicine in the past two decades, their presence in specialized levels in universities remains low.18-20
Qualitative and in-depth studies are necessary to understand the factors contributing to gender disparity in the medical field. Insights from activists in this domain will be instrumental in filling the part of the knowledge gap and utilizing these findings for policymaking and planning to achieve gender equality. This recognition, combined with accumulated knowledge, can pave the way for improving the current situation. Practical solutions for structural reform are essential to make institutions fairer and ensure individual agency beyond gender constraints. Therefore, this article aims to understand the structural aspects of gender discrimination from the perspective of medical students at the Iranian University of Medical Sciences. By relying on local knowledge, the goal is to identify ways to reduce ongoing inequalities and inform effective policy interventions.
Methods
This research adopts a critical paradigm, combining interpretative-constructive approaches. Also has used grounded theory. The primary motivation for choosing it is to access knowledge grounded in based on current reality. This method by fostering a deeper understanding, serves as a reliable guide for the thematic analysis method. Thematic analysis, a method within grounded theory, was used to classify and pattern data, leading to the development of theoretical insights. Researchers use coding and data analysis to interpret the data, and derive concepts and themes. This research was conducted from October 2023 to September 2024. sampling was used to select interviewees based on specific research criteria, such as being female, agreeing to participate, and having completed five years of medical education at the medical university. Given the research objective to gain a concrete understanding of the experiences of female medical students regarding gender discrimination, the study did not include interviews with male students and international students. The research was conducted under the Declaration of Helsinki, as revised in 2008.
Data collection techniques
The data collection method used was semi-structured individual interviews. The sample size comprised 15 participants which was determined based on the principle of data saturation, where no new themes emerged after the 13th interview. Two additional interviews were conducted to confirm saturation. The participants were female students in their sixth and seventh years of general medicine. The interviews varied in duration from 35 to 80 minutes and were conducted at locations chosen based on the participants’ preferences. At the beginning of each interview, the researcher introduced the research and the objectives of the study, provided an informed consent form, and obtained permission to record the interview while maintaining confidentiality and privacy. Participants were informed of the researcher’s contact details and assured they could withdraw from the study at any time. After the interview, the audio recordings were transcribed into written text. The transcripts were given to the participants for review and additional comments, which they could provide either in writing or orally. Any necessary supplementary information was then added to the data.
Data analysis
Data coding was performed by the principal investigator, with two other authors reviewing the process separately. The themes derived from the study were extracted directly from the context and inductively from data review and research literature. Initial codes were generated through open coding, followed by axial coding to identify relationships between categories. Final themes were derived through selective coding, ensuring a robust theoretical framework. The interview guide, included in the appendix, covers the study’s objectives, subject matter, demographic information of the interviewees, and interview questions.
Qualitative data analysis involves searching for and describing patterns within the data.21 This study employed thematic analyses, a method based on analytical induction. Through this approach, the researcher develops an analytical typology by classifying data and identifying patterns both within and outside the data. The researcher coded and analyzed the data by repeatedly reading the text to comprehend its content.
Study accuracy
Based on Guba and Lincoln’s22 criteria, this study assessed the reliability of the research findings using the following steps:
Credibility: In a credible study, data must be consistent and correlated, rather than scattered and contradictory. The researcher was involved in the subject matter for approximately two years. The angle method was employed, controlling the information and findings at the data level through four data sources: interview texts, notes, observations, and research literature.
Reliability: The researcher discussed the findings with several study participants, supervisors, consultants, and other researchers in the field, ensuring an evaluation and control of the results.
Confirmability: This criterion was established using direct quotes from participants, whose characteristics are presented in Table 1 and three-stage coding extracted from interview texts by the researcher, as detailed in Table 2.
Table 1.
Participants Information
|
Qualitative variable
|
|
Number (%)
|
| Gender |
Men |
0 (0) |
| Women |
15 (100) |
| Address |
Native |
8 (53) |
| Non-native |
7 (47) |
| Age rate |
24-28 years |
|
Table 2.
Categories and sub-categories
|
Main them
|
Sub-theme
|
Concepts
|
| Gender stereotypes |
1) The high trust and acceptance of male doctors in public belief, |
Trust in men, cultural acceptance of male doctors, patriarchal norms and values, men's freedom of action in choosing their field of expertise, men's extensive communication with each other, stereotypical image of male doctors, and normative acceptance of men as doctors. |
| 2) The low trust and acceptance of female doctors in public belief. |
Instilling fear and vulnerability in girls in the family and the educational environment, low trust in women's professional performance, imposition of housework and responsibilities for home and children, women's little time and energy for professional goals, cultural resistance to accepting and trusting female doctors. |
| Structural discriminations |
1) Gender quota law suppresses women's free access to medicine |
Passing a gender quota law and creating structural restrictions on women becoming doctors |
| 2) Gender discrimination in dormitory management |
Restrictions on the hours of entry and exit from the dormitory, inclusion in the file in case of delay, informing the family, introduction to the disciplinary committee, accusatory and interventionist behavior, disturbing mental peace and imposing anxiety and stress, reducing social respect and not respecting individuals' privacy, not accepting women's independence, unfair prejudices, verbal harassment, and insults and humiliation. |
| 3) Seducing female students “One Favor in Return for Another” |
The powerful position of men, points in the hands of men, the inferiority of female students, the sexual attraction of students, the low self-awareness of girls, the low self-confidence of girls, the lack of sexual and psychological protection training for female students, the lack of systematic monitoring of men's abuse of their superior position. |
4) Verbal and non-verbal sexual
Harassment
|
Gender stereotypes, inappropriate addresses for the position of being a doctor, insults, humiliation, mockery of girls' size and body, sexual jokes, staring and harassing looks, failure to respect individuals' privacy with remarks about how to dress and cover-up, reminders to correct their clothing in the presence of others, and failure to respect individuals' social respect. |
| 5) Physical sexual harassment as male dominance |
Unwanted physical contact, physical contact from professors or senior residents, imposing a feeling of insecurity in the work environment, and stress and psychological pressure |
| 6) Lack of a specialized Committee to handle sexual harassment complaints |
Blaming the victim, lack of emotional and psychological support for the abused, invitations to ignore and remain silent, and trivializing sexual harassment |
Transferability: Transferability refers to the applicability of the research findings. To ensure this, detailed descriptions were used to present all aspects of the research process. Comprehensive descriptions, covering every detail of the study process, were applied throughout all stages of the research findings. Quotes from various participants were included.
The codes assigned to the participants ensure their anonymity. This study adheres to all four criteria of trustworthiness and reliability. During the data collection stage, the criteria of “angle”—ensuring consistency in sources and findings—and the “negotiation approach,” which involves active interaction between the researcher and participants, were applied. In the analysis and interpretation stage, the “inferential coherence method” was used to ensure that the inferences and interpretations were consistent with the data analysis and that the inferences from different parts of the study were aligned.
Results
After analyzing the data from the interviews, two categories: “Gender stereotypes” and “structural discriminations” were identified as the main categories that perpetuate gender discrimination in women’s medical education, each of which includes its subcategories, which are mentioned below. These categories possess three main characteristics: they are external to individuals, they determine the allocation of position and relative power based on gender, and they present obstacles to women’s advancement in the medical profession. These criteria are essential in identifying the structural nature of these categories. The identified categories include: Gender Stereotypes: Participants reported a pervasive societal preference for male doctors, with female doctors facing lower trust and acceptance.
Structural discriminations:
The gender quota law that restricts women’s access to the medical profession
Gender discrimination in dormitory management
Seducing female Students “One Favor in return for another”
Verbal and non-verbal sexual harassment
Physical sexual harassment as a manifestation of male dominance
The absence of a specialized committee to handle sexual harassment complaints at the university
These categories and their subthemes are detailed in Table 2.
Gender stereotypes
1. The high trust and acceptance of male doctors in public belief
respondents under this category mentioned their experiences of lacking acceptance, trust, and professional recognition in the clinic. During their basic science courses at university, they did not feel significantly different from men at their level and were on par with them in teaching, learning, and earning grades. However, upon entering the clinical stage, they encountered different behaviors from professors and mainly from patients, indicating low acceptance, low trust, and low professional regard for female interns. One participant remarked, “I think professors accept boys more; boys have high self-confidence, even if they are inexperienced. For example, if a boy does not do something correctly, he is not blamed much and is treated fairly, and they say he has not learned yet, but girls are not treated that way.” The stereotypical image of the “male doctor” in the public’s mind prevents the rational acceptance of young women as doctors. A participant noted, “Society provides more opportunities for men and considers them more worthy of being doctors. From a conventional perspective, opportunities for women are very limited, as society has a high gender bias. Regarding professional acceptance of female doctors in fields such as surgery, a respondent stated, “People accept more men for surgical fields, and there is little belief that women can also be successful and skilled surgeons.”
2. The low trust and acceptance of female doctors in public belief
Within this main category, several subcategories emerge. The instillation of fear and a sense of vulnerability in girls within the family and educational environments hinders their ability to rely on themselves. It prevents them from making independent decisions based on their own will and interests and diminishes their courage and willingness to take risks. As one participant stated, “From childhood, the family gives you a sense of lack. When you leave the family, you are trapped in the limitations of the university and the work environment. Ah, I want to reach a place where everything will be fine, but it seems that there is no such place.”
In general beliefs, there is less trust in women doctors’ professional capabilities. A respondent noted, “People think that a man must be their doctor, and when they encounter a woman, they do not want to accept it. Girls are just nurses in people’s minds.”
The stereotype that married women doctors should primarily handle household chores and childcare leads to substantial role strain and psychological stress. This prevents them from seriously pursuing their professional goals and dedicating the necessary time and energy to professional growth. A participant stated: “Women have a lot of responsibilities, especially if they get married. Our culture is very wrong, with a lot of housework and, if they have children, the child is placed on the shoulders of the woman. The woman has to maintain her status as a doctor alongside them. It is a really difficult situation”.
Structural discrimination
1. Gender Quota law suppressing women’s access to medical education
Under this concept, respondents expressed their objections to limited access to the medical field due to their gender. They noted that if they were men, they would have been accepted into the medical field with a lower score. The gender quota law has unfairly deprived many girls of being accepted into the medical field over the past thirteen years. One respondent remarked: “I think the most important discrimination between girls and boys is the existence of a gender quota in the entrance exam. We asked both girls and boys in our class, and we saw that girls were accepted up to a rank of 500, while boys were accepted with a rank of 800. We were very upset. This is unfair. Why are girls being oppressed to such an extent?”
2. Gender discrimination in dormitory management
Under this subcategory, various concepts indicating blatant discrimination in the management of girls’ and boys’ dormitories were discovered. The most significant concept was the imposition of severe restrictions on the hours of entry and exit for women in the dormitory. If female students are late entering the dormitory, they face insulting behavior, unfair prejudice, and verbal harassment from university security or dormitory management. Additionally, latecomers are subjected to punitive measures, including being recorded in disciplinary files, having their families informed, or being referred to the disciplinary committee, which treats them as though they have committed a serious offense. This behavior by officials and the management of the girls’ dormitory has consequences such as a lack of respect for privacy, increased anxiety and stress, reduced social respect, and diminished mental and psychological well-being for female students. One respondent stated: “Entry-exit time restrictions for girls is much more severe. Even after nine pm, we are not allowed to go out, even with the permission of our guardians and families. There is a lot of insulting behavior towards girls, and the psychological pressure on us is very high.”
3. Seducing female students “one favor in return for another”
In expressing their experiences in this subcategory, respondents mentioned that they did not receive such offers from boys of the same level, but from professors or residents of the upper level. On one side of such a relationship were men with superior power and status, and on the other side, were female students who were sexually attractive. By abusing their positions, some senior professors and residents sought to establish unfair relationships and sexual abuse of female students through the granting of privileges such as easy grading, unwarranted passing, excessive leave, reduced work shifts, and fewer responsibilities and tasks in the department, Hence, they offered them open communication and invited them to their homes. One participant said: “Sometimes residents do not give professors a chance, especially in some fields, they have too much contact with girls, they give high grades, they want to attract girls to themselves. I think girls should be trained on how to protect themselves in the university environment.” Another participant added: “I did not experience it, but I saw many things. For example, a professor whose wife is not in Iran often flirts with interns and is very famous for this. He even invites the intern to his house.”
4. Verbal and non-verbal sexual harassment
There are several concepts under this central category. One of the most frequent categories mentioned in all interviews was titles and addresses that were inappropriate for a medical situation. Titles such as Ms. Baji, Mr. Doctor, Ms. Engineer, Pharmacist, Ms. Nurse, etc., are some of them. Insulting behaviors toward female students, such as making fun of their accent or body shape, sexual jokes, staring and harassing looks, not respecting individuals’ privacy, and pointing out their dress code in front of others, were examples of sexual harassment of female students mentioned in the interviews. One respondent said: “There was a lot of harassment here. I mostly experienced verbal harassment from patients; they made fun of my accent, and commented on my body and gait.” Another participant shared her observations about harassment from professors: “Some professors who are traditional and religious are extremely sensitive about the clothing of female interns and cause them to be harassed and humiliated. During visits, instead of focusing on teaching and visiting patients, they talk about a student’s clothing. This behavior is very patriarchal and misogynistic and greatly damages the privacy of individuals.”
5. Physical sexual harassment of female students
Many respondents reported that they did not personally experience physical harassment, instead often recounting the incidents faced by their friends. They described unwanted physical contact, typically initiated by men in positions of power, such as professors or senior residents. These incidents exerted significant psychological pressure on individuals, transforming the educational environment into a tense and traumatic space. One respondent shared: “I have experienced physical sexual harassment. It usually does not come from male peers but is mostly seen from residents or fellows. For instance, in one department, a senior resident would make contact whenever he passed by me. I wondered if this only happened to me or if this person had a problem. After discussing it with my friends, I realized he behaved this way with others as well.”
6. Lack of a specialized committee at the university to handle sexual harassment complaints
The most important issue for female students after facing sexual harassment on campus is the existence of an independent and specialized committee that can help reduce the harm caused by sexual harassment, compensate them, and take appropriate measures for primary and secondary prevention. The absence of such a committee at the University of Medical Sciences indicates structural indifference to this harmful issue. According to respondents, complaints of sexual harassment are currently handled mainly by the group manager and, in more severe cases, by university security. These handling paths, characterized by a lack of emotional and psychological support, invitations to ignore and remain silent, belittling of sexual harassment, criminalizing the harassed person, and blaming the victim, not only fail to reduce harm but also cause further damage. One participant said: “Complaints of sexual harassment are reported to the group manager, but most of the time they are not taken seriously. Even if someone complains to security, unfortunately, they are mostly blamed. Most of the time they say, ‘Look what you did to deserve this treatment.’ That’s why people keep quiet because instead of supporting people, they insult and blame them, and this makes people afraid and more silent.”
The grounded theory
A central phenomenon is a category that provides meaning and function to other categories concerning it. In this study, the category of “Struggle between agency and discrimination” was identified as the central phenomenon. The rejection of this category is evident in all the data. This central phenomenon suggests that some female interns, despite facing various forms of discrimination and gender stereotypes at both structural and interpersonal levels, also consider their agency, influenced by their personality traits and gender socialization. Some of them rely on their conditional autonomy to combat certain discriminations. Although they may hold weaker academic positions, some have realized that through increased hard work, effort, and personal and professional growth, they can contribute to improving the situation in some instances.
The causal conditions creating this central phenomenon include:
Gender stereotypes: The high trust and acceptance of male doctors in public belief, The low trust and acceptance of female doctors in public belief.
Structural discrimination in-laws and management: The gender quota law that limits women’s free access to medicine, gender discrimination in the management of dormitories, seducing female students by offering favors in return, verbal, non-verbal, and physical sexual harassment, lack of specialized committee in the university to handle sexual harassment complaints.
The intervening factors in the formation of this central phenomenon include:
Field of action: Hospital, medical university
Reproducibility of discrimination experiences
Ethnic background
The underlying factors creating this central phenomenon are:
Individual capability
Agency and praxis
The interactions and strategies that activists exhibit as a result of this situation include: “A spectrum from passivity to agency”.
Ultimately, the central phenomenon and the strategies that students employ lead to the following consequences:
Suppression of capabilities & self-efficacy
Psychological & mental stress
Low professional advancement
Sexual and psychological harms
Academic exhaustion
Tendency to migrate
The findings are presented in Figure 1.
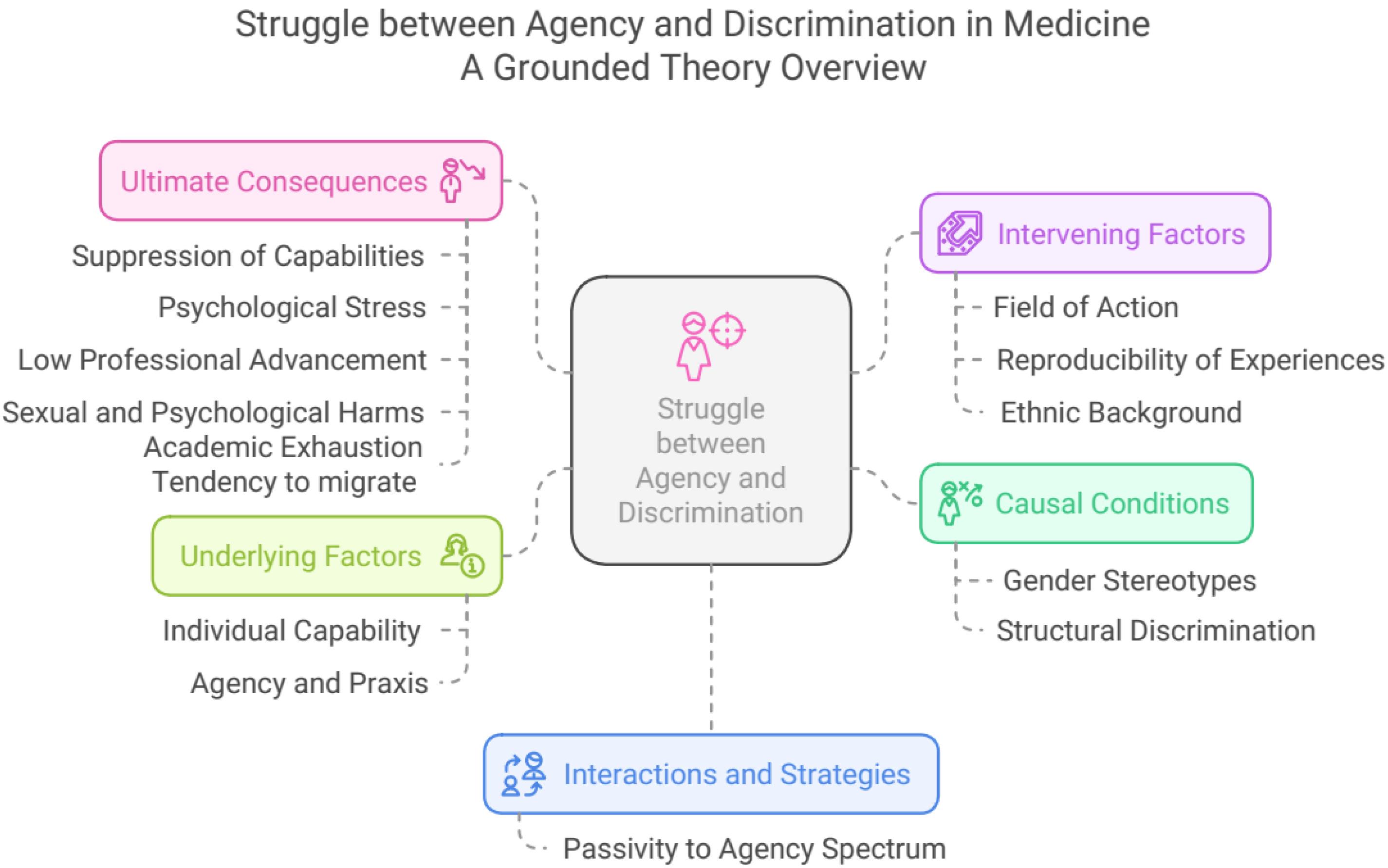
Figure 1.
A Grounded Theory Overview
.
A Grounded Theory Overview
Analysis of context with process
The pathways and activities through which learners acquire knowledge are gendered. This gendered context is evident in norms, values, structural aspects of laws and regulations, and the allocation of opportunities and facilities.23 The central phenomenon identified in this research is the “struggle between agency and discrimination.” Various conditions and their consequences are outlined below. Women often choose the medical field due to basic education, encouragement from families and teachers, and their interest in achieving distinguished academic and professional positions. They view medicine as a platform for realizing their existential capabilities, aiming for high scientific and status positions, earning an income, and gaining independence to create a new societal identity.
However, in this field of action, women encounter numerous structural and cultural obstacles implying discrimination against their male peers. Firstly, women face gender quotas for medical admission, imposing unequal access because the number of women taking the medical entrance exam is higher than that of men, creating significant barriers. Additionally, students living in dormitories face restrictive, oppressive, and discriminatory management methods between girls’ and boys’ dormitories. Women experience severe restrictions on entering and leaving the dormitory, questioning their freedom and independence. Non-compliance results in disciplinary actions, including being summoned to the disciplinary committee.
The presence of powerful and authoritative men (professors and residents) with numerous privileges, alongside women with high sexual attractiveness and low status as students, creates an environment conducive to student exploitation, offering favors in exchange for benefits. Consequently, students face numerous instances of sexual abuse for various privileges, including verbal, non-verbal, and physical sexual harassment. The absence of a specialized committee to handle sexual harassment complaints further highlights the gendered nature of university structures. Gender stereotypes, including high trust and acceptance of male physicians and low trust and acceptance of female physicians’ capabilities, also contribute to the central phenomenon of this research.
Contextual conditions, converging at specific times and places, include the field of practice (hospital and university), the diversity and repetition of discriminatory experiences among individuals, and ethnic background (intensifying gender discrimination). Mediating factors mitigate or change these causal conditions. Individual capabilities such as self-confidence, risk-taking, boldness, fearlessness, and studiousness play crucial roles. Agency and praxis, emphasizing bounded autonomy and conditional self-determination, are essential. Human action is based on subjective choices, reasons, free will, agency, and rationality within structural or cultural limits. Praxis, the core of human beings, involves the conscious ability to transform society and the environment, leading to self-understanding and the elimination of alienation.
Consequently, individuals choose strategies on a “spectrum from passivity to agency” based on intermediary conditions and discriminatory experiences. Ultimately, these conditions and strategies result in various outcomes. Female students, facing various types of discrimination in their educational environment, experience suppressed self-efficacy and academic and professional capabilities, severe psychological stress, disrupted professional development, and potential psychological and sexual harm. They may face academic burnout and its consequences, and consider emigrating to seek more equitable educational or employment structures.
Discussion
This study identified key structures perpetuating gender discrimination in medical education. Through interviews with female students in their final year of general medicine, two main categories and eight sub-categories were identified. Some of these categories, such as the societal acceptance of male physician superiority and the existence of gender stereotypes that hinder women’s professional growth, are emphasized in Tavakol et al20 study. They demonstrated that the acceptance of societal gender stereotypes negatively impacts girls’ professional growth, their continuation of education, and their attainment of senior management positions, aligning with some findings of this study. Similarly, Vedadhir et al19 highlights the existence of gender stereotypes as obstacles to women’s academic and professional growth. Gender stereotypes have been shown to cause gender-based social exclusion and deny women equal opportunities for advancement in the medical education system. Kazemi18 further asserts that women have historically struggled to enter medical schools and, despite their success in doing so, continue to face gender discrimination and inequalities. This includes the gender-based wage gap and lack of advancement opportunities for women in Iran. These findings, consistent with this study, conclude that opportunities and facilities in medicine are not equally distributed between men and women, with men having more opportunities and facilities.
In addition to the similarities with previous Iranian studies, this study added new insights. These include the existence of discriminatory laws affecting access to the medical field between genders, the application of gender quotas to the detriment of women, gender discrimination in the management of dormitories and university security, and unequal gender management approaches within universities. Furthermore, the lack of an official authority to handle sexual harassment complaints, the presence of sexual harassment in medical education environments, and the phenomenon of quid pro quo, as reported by participants, are prevalent in professional and academic settings.
European studies in this field are more diverse, advanced, and innovative. For example, the Gender in Higher Education Project in French universities (2014) showed that, despite structural measures, gender-based inequalities persist. Rogers and Molinier24 points to institutional resistances that produce anthropocentric biases and gender norms, which are sources of discrimination. This study emphasizes the “glass ceiling” preventing women from advancing in their careers and education at universities. Furthermore, they note the need to explore the complex interactions between gender and male-dominated norms and to address norms to avoid gender-based prejudices and consider their effects in designing equality action plans.
From a broader perspective, comparing European studies on gender discrimination with domestic research reveals that both groups acknowledge the existence and significance of gender discrimination in universities and the medical field. They highlight it as a fundamental problem requiring effective solutions at various levels. However, a key distinction is that studies have achieved a higher level of depth, knowledge accumulation, and progress. Extensive projects within these studies address the underlying structural issues, causes, factors, and characteristics of gender discrimination in academic settings.
For instance, the “Gender Time”,25 funded and implemented by the European Commission from 2013 to 2016, aimed to identify the best systemic approaches for action plans promoting equality and increasing the representation and professional advancement of women professors and researchers. Also, emphasize the need to explore the complex interactions between gender and superiority norms and to address gender-based prejudices. In another major study conducted in German universities, researchers observed changes at both organizational and individual levels following the implementation of gender equality laws. Although professional opportunities for women in academia have improved and gender equality laws have been enacted, women remain a minority, and career-related barriers persist, perpetuating inequalities.24
Research on gender inequality in Europe indicates that institutional changes are ongoing, and effective measures have been prepared from an institutional and legal perspective to create equal opportunities for women in academia, teaching, and research. Various projects are being conducted to monitor and evaluate the effectiveness of these laws and identify strengths and weaknesses to promote equality measures at the institutional level. Developed countries recognize the importance of human equality for societal development and individual well-being. Thus, they focus on institutional solutions and complementary studies to address obstacles. Based on the findings of this research: Three key features are identified in research conducted in developed societies, particularly in Europe: (1) acceptance of gender discrimination as an issue, (2) implementation of legal and regulatory measures, and (3) monitoring and identifying gaps and flaws in these laws to create institutional changes for gender equality. These steps reflect an institutional will to achieve equality regardless of gender.
In Iran, however, the prerequisite for institutional changes is the acceptance of structural discrimination, which remains a contentious issue. Conflicting views in parliament and government regarding the existence of discrimination hinder progress and alignment on institutional changes at the legislative and policy-making levels. Research in Iran is not conducted under broad, institutionally supported projects but rather sporadically based on researchers’ interests. Consequently, Iranian research is still focused on proving the existence of gender discrimination and highlighting the need for institutional action.
For example, Falahati26 in her study on gender justice, points out the existence of structural obstacles to women’s professional growth in universities. These structural inequalities suppress women despite their new identities. The lack of infrastructure and socio-economic capacities to support educated women and the neglect of their identity needs for professional development result in dissatisfaction and feelings of weakness among half of society, posing a significant obstacle to sustainable development in Iran
Conclution
This research offers a deeper understanding of the structural aspects of gender discrimination in medical education. By addressing specific issues within the field, it provides practical suggestions for improving conditions and reforming the medical education system to eliminate gender discrimination, drawing on sociological knowledge and a critical approach. The findings of this study may be transferable to other medical education settings in similar cultural contexts, particularly in regions where gender discrimination is prevalent. However, further research is needed to explore the applicability of these findings in different cultural and institutional settings.
Suggestions
Given that gender discrimination has developed over an extended period and is influenced by various factors, particularly cultural backgrounds, its elimination or reduction requires time and multifaceted measures. In light of existing studies and actions taken by various societies to mitigate discrimination, the following recommendations are proposed for advancing gender equality in academic and organizational settings. For instance, in Germany, gender equality legislation was first enacted by legislative bodies. This was followed by implementation across various organizations, including universities, where changes were monitored at both organizational and individual levels by researchers. They scrutinized the allocation of professional opportunities between women and men. Similarly, in France, the extensive project titled “The Gender Time” aimed to develop systematic solutions for implementing action plans to foster equality. The goal was to increase the representation of women professors and researchers and to promote their careers. These projects highlighted the necessity of examining the intricate interplay between gender, norms, and organizational practices while legal equality measures were enacted. In these contexts, gender issues and their interactions with other social concepts are key concerns for policymakers and researchers. Significant resources and budgets support institutional reforms aimed at addressing these challenges. Drawing on the strategies employed in these societies, alongside the findings from current research and other studies in this field, the following suggestions are made to enhance the situation in Iranian society. These recommendations take into account the existing contexts and capacities within Iran. However, the following procedures may facilitate and accelerate this process to some extent:
Re-examining the gender quota law and abolishing the gender quota.
Establishing a specialized committee to address complaints regarding discrimination based on gender, ethnicity, language, and culture.
Establishing a specialized research and development (R&D) committee to implement structural reforms with the necessary scientific support to create equal opportunities and facilities for women and men. This may include positive discrimination in some cases to allocate resources and opportunities more fairly for women.
Changing the management procedures of dormitories and eliminating the time restrictions for women’s entry and exit from student dormitories.
Implementing a gender quota for appointing management positions or recruiting faculty members at the university.
To implement the suggested policy changes, universities could establish task forces to monitor gender equality initiatives, provide training for faculty and staff on gender sensitivity, and create support systems for students who experience discrimination.
Future research should explore the long-term impact of gender discrimination on women’s career trajectories in medicine, as well as the effectiveness of interventions aimed at reducing gender disparities in medical education.
Limitations
This study has several limitations. First, the sample was limited to female students at one university, which may limit the generalizability of the findings. Second, the reliance on self-reported data may introduce bias, as participants may underreport experiences of discrimination due to fear of repercussions. Future research should include a more diverse sample and explore the perspectives of male students and faculty members.
Competing Interests
The authors report no conflict of interest.
Ethical Approval
To ensure confidentiality, all identifying information was removed from transcripts, and participants were assigned pseudonyms. Audio recordings were securely stored and deleted after transcription.
All participants provided written informed consent before the interviews began. No personal identifiers were recorded to ensure the participants’ anonymity. This study was reviewed and approved by the Ethics Committee at Kharazmi University of Tehran, under the ethics code IR.KHU.REC.1402.131.
Acknowledgements
This article is part of the findings of a doctoral dissertation in sociology. I would like to express my sincere gratitude to my supervisor, Professor Fatemeh Javaheri, and my advisor, Professor Alizadeh, for their deep and valuable knowledge that assisted me in conducting this research. I also extend my thanks to the Vice Chancellor for Research at Kharazmi University of Tehran, the Vice Chancellor for Research and Technology at the University of Medical Sciences where the research is conducted, and the General Security Department of this University of Medical Sciences for issuing the necessary permits to conduct this research. Finally, I am deeply grateful to all the participants in this research who generously shared their experiences and perspectives during the interview sessions.
References
- Kronsell A. Homeless in academia: homesteading as a strategy for change in a world of hegemonic masculinity. In: DiGeorgio-Lutz J, ed. Women in Higher Education: Empowering Change. Praeger; 2002.
- Pololi LH, Jones SJ. Women faculty: an analysis of their experiences in academic medicine and their coping strategies. Gend Med 2010; 7(5):438-50. doi: 10.1016/j.genm.2010.09.006 [Crossref] [ Google Scholar]
- Fox G, Schwartz A, Hart KM. Work-family balance and academic advancement in medical schools. Acad Psychiatry 2006; 30(3):227-34. doi: 10.1176/appi.ap.30.3.227 [Crossref] [ Google Scholar]
- Eitzen DS, Zinn MB, Smith KE. Social Problems. 12th ed. Pearson College Div; 2012.
- Acker J. Inequality regimes: gender, class, and race in organizations. Gend Soc 2006; 20(4):441-64. doi: 10.1177/0891243206289499 [Crossref] [ Google Scholar]
- Leaper C, Friedman CK. The socialization of gender. In: Grusec JE, Hastings PD, eds. Handbook of Socialization: Theory and Research. New York: The Guilford Press; 2007. p. 561-87.
- Jendretzky K, Boll L, Steffens S, Paulmann V. Medical students’ experiences with sexual discrimination and perceptions of equal opportunity: a pilot study in Germany. BMC Med Educ 2020; 20(1):56. doi: 10.1186/s12909-020-1952-9 [Crossref] [ Google Scholar]
- Barbier JM, Carrard V, Schwarz J, Berney S, Clair C, Berney A. Exposure of medical students to sexism and sexual harassment and their association with mental health: a cross-sectional study at a Swiss medical school. BMJ Open 2023; 13(4):e069001. doi: 10.1136/bmjopen-2022-069001 [Crossref] [ Google Scholar]
- Velin L, Chew MS, Pompermaier L. Discrimination in an “equal country”-a survey amongst Swedish final-year medical students. BMC Med Educ 2022; 22(1):503. doi: 10.1186/s12909-022-03558-6 [Crossref] [ Google Scholar]
- Faria I, Campos L, Jean-Pierre T, Naus A, Gerk A, Cazumbá ML. Gender-based discrimination among medical students: a cross-sectional study in Brazil. J Surg Res 2023; 283:102-9. doi: 10.1016/j.jss.2022.10.012 [Crossref] [ Google Scholar]
- Kristoffersson E, Andersson J, Bengs C, Hamberg K. Experiences of the gender climate in clinical training - a focus group study among Swedish medical students. BMC Med Educ 2016; 16(1):283. doi: 10.1186/s12909-016-0803-1 [Crossref] [ Google Scholar]
- Babaria P, Abedin S, Berg D, Nunez-Smith M. “I’m too used to it”: a longitudinal qualitative study of third year female medical students’ experiences of gendered encounters in medical education. Soc Sci Med 2012; 74(7):1013-20. doi: 10.1016/j.socscimed.2011.11.043 [Crossref] [ Google Scholar]
- Heffron AS, Braun KM, Allen-Savietta C, Filut A, Hanewall C, Huttenlocher A. Gender can influence student experiences in MD-PhD training. J Womens Health (Larchmt) 2021; 30(1):90-102. doi: 10.1089/jwh.2019.8094 [Crossref] [ Google Scholar]
- Kawase K, Carpelan-Holmström M, Kwong A, Sanfey H. Factors that can promote or impede the advancement of women as leaders in surgery: results from an international survey. World J Surg 2016; 40(2):258-66. doi: 10.1007/s00268-015-3332-x [Crossref] [ Google Scholar]
- Brown E. California Professor, Writer of Confidential Brett Kavanaugh Letter, Speaks Out About Her Allegation of Sexual Assault. The Washington Post; 2018.
- Jagsi R, Griffith KA, Stewart A, Sambuco D, DeCastro R, Ubel PA. Gender differences in the salaries of physician researchers. Jama 2012; 307(22):2410-7. doi: 10.1001/jama.2012.6183 [Crossref] [ Google Scholar]
- Whitworth JA. Women and global health: a personal view. Glob Health Epidemiol Genom 2016; 1:e10. doi: 10.1017/gheg.2016.6 [Crossref] [ Google Scholar]
- Kazemi S. Women in Modern Medicine. publication: Author in collaboration with Damon Publication, Tehran; 2023. [Persian].
- Vedadhir A, Hani Sadati SM, Nourbakhsh SM. The obstacles of women’s professional promotion in medical education system of Iran: a qualitative study in the sociology of medical education. Cultural Studies & Communication 2013;9(31):11-41. [Persian ].
- Tavakol M, Javadi-Yeganeh MR, Hani Sadati SM. A sociological study on women’s status in Iran’s medical education system. Woman in Development & Politics 2011;8(4):27-50. [Persian ].
- Neuman WL. Basics of Social Research: Quantitative and Qualitative Approaches. 3rd ed. London: Allyn & Bacon; 2007.
- Guba E, Lincoln YS. Naturalistic Inquiry. Beverly Hills, CA: Sage Publications Ltd; 1985.
- Fox Keller E. Gender and science. Psychoanalysis and Contemporary Thought 1978; 1(3):409-33. [ Google Scholar]
- Rogers R, Molinier P. Les femmes dans le monde académique. Perspectives comparatives. Rennes (Presses universitaires de); 2016; 239-348. [French].
- Gender time website. Available from: https://gendertime.org/.
- Falahati L. Gender Justice in Higher Education in Iran. Tehran: Institute of Cultural and Social Studies; 2019.