Res Dev Med Educ. 14:33309.
doi: 10.34172/rdme.025.33309
Original Article
Innovative education in antibiotic stewardship program among undergraduate medical students: A card game-based approach
Santhosh Samuel Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft, Writing – review & editing, 
Wilfred Premila Magdalene Data curation, Investigation, Methodology, Resources, Writing – review & editing,
Eldhose Anupa Data curation, Methodology, Resources, Writing – review & editing,
Arokyaraj Blessana Mary Data curation, Methodology, Resources, Writing – review & editing,
Raja Priya Data curation, Methodology, Resources, Writing – review & editing,
Margaret Shanthi Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing, , *
Author information:
Department of Pharmacology and Clinical Pharmacology, Christian Medical College, Vellore
Abstract
Background:
Antibiotic resistance, a pressing global issue, is particularly severe in India due to high antibiotic use and poor prescribing practices. Undergraduate medical education often lacks focus on antimicrobial stewardship, leaving future prescribers unprepared. This study evaluates an innovative card game designed to enhance learning about antibiotics among medical students.
Methods:
This study involved 100 medical students, randomized into two groups: one engaged with an antibiotic-themed card game, and the other received a lecture. The game, featuring 30 antibiotics, was designed to teach stewardship through interactive play. Knowledge was assessed via pre-and post-tests. Feedback was also collected from the students.
Results:
The card game group significantly improved in post-test scores (P<0.0001). However, the final scores were comparable to the lecture group (P=0.5273). Notably, the card game significantly enhanced student engagement, with the majority reporting an improved understanding of antibiotic spectrum, toxicity, and unique attributes like coverage for drug-resistant organisms.
Conclusion:
The card game enhanced engagement, suggesting its utility in antimicrobial stewardship education. This method of interactive learning has the potential to augment medical education, equipping students to navigate the complexities of antibiotic prescribing amidst increasing resistance.
Keywords: Antibiotics, Resistance, Stewardship, Students, Activity
Copyright and License Information
© 2025 The Author(s).
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, as long as the original authors and source are cited. No permission is required from the authors or the publishers.
Funding Statement
Funding was provided by the fluid research grant,Institutional Review Board, Christian Medical College, Vellore, Grant number: 2407136 dated 24/7/2024.
Introduction
Antibiotic resistance is recognized as a formidable challenge to global public health.1 Over the past few decades, the misuse of antibiotics has contributed to the development of multidrug-resistant bacteria,2 thereby escalating the cost and complexity of treating numerous infections, rendering some infections untreatable. Antimicrobial resistance (AMR) undermines treatment effectiveness, causing chronic infections and heightened pathogen transmission.3
India, as the world’s largest consumer of antibiotics by volume,4 faces exacerbated issues due to suboptimal prescription practices.5 Research highlights the frequent, unwarranted use of broad-spectrum antibiotics in the absence of confirmed bacterial infections,6 a practice that significantly correlates with the high prevalence of antibiotic resistance in bacteria responsible for common infections within the country.7
Despite the growing recognition of Antimicrobial Stewardship Programs, educational efforts in this area predominantly focus at postgraduate levels.8,9 In contrast, undergraduate medical education on antimicrobial stewardship has been relatively overlooked.10,11 A survey conducted among medical students nearing graduation indicated that only a third felt proficient in antimicrobial prescribing principles, with a significant majority expressing a desire for more education in this domain.11 Incorporating antimicrobial stewardship education into undergraduate curricula offers a substantial potential for influencing future prescribing behaviors, especially since these habits are most pliable during the initial phases of medical training.12-14
Medical education has increasingly embraced interactive teaching methods, such as problem-based learning (PBL), simulation-based training (SBL), and case-based learning (CBL) to enhance engagement and knowledge retention.15-17 These approaches have proven effective in fostering critical thinking and practical skills among students. However, there remains a gap in innovative tools specifically designed to teach complex topics like antibiotic mechanisms and stewardship. To address this, we developed a set of educational cards, adapted from existing antibiotic-themed card designs,18 and an assessment was conducted to evaluate the effectiveness of these cards as an educational tool within this demographic. The cards also displayed the mechanism of action of the drug and other key concepts.
Materials and Methods
Study design and setting
This was a prospective randomized controlled trial done as part of an Antibiotic Stewardship Programme. All the students were included in this study after written informed consent and the study was carried out after clearance from Institutional Review Board – IRB Minute Number 2407136. Thirty antibiotics were chosen for the cards, and 50 students were divided into 10 groups with 5 students in each group supervised by a faculty member. The faculty member elucidated the game’s rules, and the game was conducted thrice to ensure students were thoroughly familiar with all the cards and their attributes. Additionally, students were allotted time to examine all the characteristics of the cards before engaging in gameplay. A 20-item MCQ based on the antibiotics chosen for the activity was given before and after the card game activity and didactic lecture.
Randomization
Participants were allocated to one of two groups using simple randomization based on a computer-generated list of random numbers, created with Statistical Analysis System Software. Group 1 (n = 50) was allotted to play the card game and group 2 (n = 50) was asked to attend the didactic lecture. Each participant was randomly assigned without blinding. The faculty members who evaluated the test results were independent of the study and were blinded to both the participants and their respective groups. Similarly, the statisticians who analyzed the study data were also blinded to the identities of the participants and the groups.
Results
A card game, modelled after the work done by Davies18 on antibiotics, was developed. This game featured a selection of 30 antibiotics (Table 1) from the WHO AWaRe (ACCESS, WATCH, RESERVE) classification.
Table 1.
The antibiotics chosen for the card activity
|
Access
|
Watch
|
Reserve
|
Amoxicillin + Clavulinic acid
Ampicillin + Sulbactam
Cloxacillin
Cephalexin
Doxycycline
Nitrofurantoin
Gentamicin
Amikacin
Clindamycin
Co-Trimoxazole
Metronidazole |
Piperacillin + Tazobactam
Cefuroxime
Cefotaxime
Ceftriaxone
Vancomycin
Meropenem
Azithromycin
Clarithromycin
Erythromycin
Ciprofloxacin
Moxifloxacin
Levofloxacin
Norfloxacin
Rifampicin |
Ceftazidime + Avibactam
Ceftaroline Fosamil
Linezolid
Tigecycline
Polymyxin B |
-
ACCESS: First-choice antibiotics for common infections, promoting rational use.
-
WATCH: Higher resistance potential, to be used more cautiously.
-
RESERVE: Last-resort treatments for multidrug-resistant infections.
The AWaRe classification serves as an instrument for tracking antibiotic usage, establishing benchmarks, and evaluating the outcomes of stewardship initiatives designed to enhance antibiotic utilization and mitigate AMR.19
The antibiotics were chosen to focus on their activity against critical, high, and moderate priority pathogens as listed WHO updated bacterial priority pathogens list 2024 from around the globe and from India as suggested by the Indian Council of Medical Research.20,21
Each card depicted an antibiotic, assigning scores based on its spectrum against Gram-positive and Gram-negative bacteria, reflecting contemporary clinical challenges in India (the score points correspond to the number of prevalent, clinically significant bacteria targeted) based on the Indian pathogen priority list.22,23 The scores allotted for every antibiotic were based on the criteria given in Table 2. The scoring was meticulously determined with input from infectious disease specialists and microbiologists, with higher scores indicating greater significance or severity associated with the antibiotic’s characteristics. The cards were designed in such a way as to give more importance to commonly used drugs like Polymyxin B which had a very high score for superpower to drive home the point to the students that we should be prudent in choosing the antibiotics as we are running out of them. The cards were crafted to emphasize critical medications such as Polymyxin B, which received a significantly high score for its ‘superpower’ attribute, thereby underscoring to students the necessity for judicious antibiotic selection, given the dwindling availability of effective options.
Table 2.
Scoring criteria for antibiotic card activity
|
Criteria
|
Scores allotted
|
| Route of administration |
|
| Oral |
2 |
| Intravenous |
6 |
| Toxicity |
|
| Severe or highly significant |
1 |
| Less severe or less significant |
0.5 |
| AWaRe classification |
|
| ACCESS group of antibiotics |
1 |
| WATCH group of antibiotics |
10 |
| RESERVE group of antibiotics |
20 |
| Superpowers |
|
|
Enterococcus
|
5 |
Multidrug-resistant or extensively drug-resistant
tuberculosis |
10 |
Methicillin-resistant Staphylococcus aureus (MRSA) or
vancomycin-resistant Staphylococcus aureus (VRSA) or
vancomycin-resistant enterococci (VRE) |
15 |
| Drug-sensitive tuberculosis |
20 |
|
Pseudomonas
|
20 |
|
Acinetobacter
|
25 |
| Drug-resistant Escherichia coli |
25 |
|
Klebsiella
|
25 |
Scoring rationale
The scoring system was crafted to mirror clinical priorities in antibiotic stewardship, with numerical values assigned to reflect relative importance and urgency in prescribing decisions, as validated by two infectious disease specialists and one microbiologist from Christian Medical College, Vellore. Over three meetings, they calibrated scores using WHO AWaRe guidelines, Indian resistance patterns,22,23 and educational goals, ensuring higher numbers signaled greater clinical weight. The justification for each category’s numbers is as follows:
-
Route of administration: Oral antibiotics were assigned 2 points as a baseline, reflecting their common use in mild, outpatient infections (e.g., amoxicillin for otitis media). Intravenous (IV) antibiotics scored 6—three times higher—to emphasize their threefold greater potency, systemic reach, and association with severe, often hospital-treated infections (e.g., meropenem for sepsis). This 1:3 ratio was chosen to teach students the escalation from routine to critical care.
-
Toxicity: Less severe toxicity (e.g., nausea with erythromycin) scored 0.5, a minimal value to note manageable risks. Severe toxicity (e.g., nephrotoxicity with Polymyxin B) scored 1—double the value—to reflect its doubled impact on clinical decisions, balancing efficacy against safety concerns, a key stewardship lesson.
-
AWaRe classification: ACCESS antibiotics (e.g., amoxicillin) scored 1 as the lowest value, promoting their routine use per WHO’s 60% target for low-resistance options.19 WATCH antibiotics (e.g., ciprofloxacin) scored 10—tenfold higher—to signal a significant jump in resistance risk and need for caution, aligning with their restricted use in India’s high-resistance context. RESERVE antibiotics (e.g., ceftazidime-avibactam) scored 20—double WATCH—to underscore their twice-as-critical status as last-resort options, reflecting their rarity and priority in MDR infections. This 1:10:20 progression mirrors AWaRe’s escalating stewardship hierarchy.
-
Superpowers: Scores ranged from 5 to 25 to prioritize resistant pathogens’ clinical burden. Enterococcus (5) received a low score as a moderate challenge often managed with ACCESS drugs. MDR/XDR tuberculosis (10) doubled this, reflecting its complexity, while MRSA/VRSA/VRE (15) increased further due to rising prevalence. Drug-sensitive TB and Pseudomonas (20) shared a high score for their global/local burden, and Acinetobacter, drug-resistant E. coli, and Klebsiella (25) topped the scale—five times Enterococcus—as critical MDR threats in India, per ICMR data.22 This 5-point increment (5, 10, 15, 20, 25) was set to rank pathogens by resistance severity and treatment urgency, validated by specialists’ consensus.
Specialists ensured scores aligned with real-world prescribing challenges (e.g., Polymyxin B’s 25 for Acinetobacter reflects its last-line necessity in ICUs), adjusting initial drafts (e.g., reducing MDR-TB from 15 to 10 to differentiate from MRSA) based on ICMR resistance prevalence and WHO priority lists. This numerical framework taught students to weigh accessibility (route), risks (toxicity), resistance potential (AWaRe), and pathogen severity (superpowers), embedding stewardship principles in gameplay.
Card game mechanics
The card game, styled after ‘Trump Cards’®, was designed as a competitive, interactive learning tool for second-year medical students. A deck of 30 unique antibiotic cards was distributed equally among 5 players per group (6 cards each), supervised by a faculty member. The game proceeded as follows:
-
Purpose: Players aimed to collect the most cards by winning rounds based on strategic attribute comparisons.
-
Rules:
-
The starting player selected one attribute from their top card (e.g., spectrum score, toxicity, superpower) and announced its value (e.g., “Superpower: 25”).
-
Other players revealed the same attribute from their top cards. The highest value won the round, with the winner collecting all played cards. Ties were resolved by comparing a second attribute chosen by the initial player (e.g., AWaRe score).
-
Play rotated clockwise, with each player choosing an attribute for the next round.
-
Gameplay: A round ended when all cards were played, or a player collected all cards. The game was conducted thrice per group (approximately 20 minutes per session), allowing students to cycle through the deck and reinforce learning. Before gameplay, students had 10 minutes to review all card attributes (e.g., mechanism of action, clinical use) with faculty guidance.
-
Interaction dynamics: Players discussed choices aloud (e.g., “I’ll use Polymyxin B’s superpower for Pseudomonas”), prompted by faculty to explain rationales (e.g., “Why is this a reserve group drug?”), fostering peer-to-peer teaching and critical thinking about stewardship principles (e.g., avoiding overuse of RESERVE antibiotics).
Study implementation
The activity was part of an Antibiotic Stewardship Programme for 100 second-year students, randomized into two groups (n = 50 each) using a computer-generated list (Statistical Analysis System Software). Group 1 played the card game, supervised by faculty who explained rules and facilitated discussions, while group 2 received a 45-minute didactic lecture covering the same antibiotic content via slides. Pre- and post-tests (20-item MCQs) assessed knowledge, with faculty evaluators and statisticians blinded to group assignments.
Statistical analysis
Sample size justification
While a formal power calculation was not conducted, our sample size of 100 participants (50 per group) was determined based on pragmatic considerations, including cohort availability and feasibility within the curriculum timeframe. Using observed data (mean difference = 0.32, pooled SD = 3.0), this sample achieves 80% power (α = 0.05, two-tailed) to detect a Cohen’s d = 0.4 (small-to-medium effect), which is educationally meaningful for knowledge gains.
Data was expressed as Mean ± SD. Paired t-test was conducted to compare the pre and post-test marks of both the groups. An unpaired t-test was done to compare the post-test marks of group 1 and group 2 using GraphPad Prism version 10.0.0 for Windows, GraphPad Software, Boston, Massachusetts, USA. Descriptive statistics was used for qualitative data.
Discussion
The introduction of an antibiotic-themed card game within the antimicrobial stewardship curriculum represents a notable progression in medical education, specifically targeting the issue of AMR at the undergraduate level, where traditional didactic lectures predominantly prevail. This study illustrates that innovative approaches can function not merely as educational aids but as transformative strategies for enhancing comprehension of antibiotic usage and stewardship principles among future medical professionals.
The card game group (Group 1: Table 3) demonstrated a statistically significant improvement in post-test scores, indicating a substantial enhancement in knowledge retention and application. This outcome contrasts with the didactic lecture group (Group 2: Table 4), where the improvement was not statistically significant but the pre-test scores in this group were a touch higher. This suggests that the interactive nature of the card game, which encourages active learning through competition and immediate feedback, may be more effective in fostering a deeper understanding of complex topics like antibiotic stewardship.
Table 3.
Group 1 (card based activity)
|
|
Pre test
|
Post test
|
P
value
|
| Mean |
12.08 |
15.03 |
0.0001 |
| SD |
3.19 |
2.03 |
Table 4.
Group 2 (didactic lecture)
|
|
Pre test
|
Post test
|
P
value
|
| Mean |
13.69 |
14.71 |
0.0977 |
| SD |
3.91 |
3.73 |
In evaluating the knowledge of reserve antibiotics and their unique capabilities in targeting highly resistant organisms, students in group 1, who engaged with the card-based activity, demonstrated superior performance compared to those in group 2, who received a didactic lecture. This was supported by statistically significant p-values of 0.0338 for reserve antibiotics knowledge (Table 5) and 0.0026 for understanding the ‘superpowers’ of antibiotics (Table 6). However, a comparison of post-test results between the two groups (Table 7) revealed that while group 1 exhibited a slight trend toward improvement, the mean scores remained comparable. The P value of 0.5273 indicates that this difference was not statistically significant. This difference suggests that while the card game was successful in enhancing knowledge among its group, it did not outperform the lecture method in achieving final knowledge outcomes.
Table 5.
Question on the knowledge area of reserve antibiotics from AWaRe classification; antibiotic-themed card game vs didactic lecture
|
|
Correct responses
|
Incorrect responses
|
Two tailed
P
valuea
|
| Group 1 (card based activity) |
43 |
7 |
0.0338 |
| Group 2 (didactic lecture) |
33 |
17 |
a Fisher’s exact test used to test significance.
Table 6.
Question on the knowledge area of superpowers: antibiotic-themed card game vs didactic lecture
|
|
Correct responses
|
Incorrect responses
|
Two tailed
P
valuea
|
| Group 1 (card based activity) |
41 |
9 |
0.0026 |
| Group 2 (didactic lecture) |
26 |
24 |
a Fisher’s exact test used to test significance.
Table 7.
Antibiotic-themed card game vs didactic lecture
|
|
Post-test of group 1
|
Post-test of group 2
|
P
value
|
| Mean |
15.03 |
14.71 |
0.5273 |
| SD |
2.03 |
3.73 |
This equivalence in knowledge gains, paired with heightened engagement, positions the card game as a complementary tool rather than a replacement for lectures. Didactic lectures remain effective for structured content delivery, as evidenced by group 2’s solid performance, but often lack the dynamic interaction inherent in the card game. The game’s design, rooted in the WHO AWaRe classification and Indian pathogen priorities, distilled essential antibiotic knowledge into a competitive format, encouraging critical thinking about judicious use—a key stewardship tenet. However, the comparable final scores between groups may reflect the limited duration of exposure (three sessions) and the modest sample size (n = 100), alongside students’ greater familiarity with lecture-based learning.
The novelty of the card game approach in teaching antimicrobial stewardship to undergraduate medical students lies in its targeted focus on a critical yet often underrepresented area of medical education, distinguishing it from broader interactive methods such as simulations, CBL, and PBL. While simulations demand substantial resources and infrastructure, and CBL and PBL require the development of intricate clinical scenarios to address specific antibiotic use—particularly in cases of drug-resistant or complex infections—the card game distills essential antibiotic knowledge into an engaging, competitive format. This innovative approach not only complements existing teaching strategies but also provides a practical and accessible solution to foster a deeper understanding of antimicrobial stewardship among future healthcare professionals.
The design of the cards and the scoring system, as previously outlined, was meticulously crafted following an extensive review of literature concerning priority pathogens both globally and specifically within India, alongside guidelines for their treatment. This was achieved with input from infectious disease specialists and microbiologists, focusing on antibiotics deemed essential for undergraduate medical students. Furthermore, the antibiotics were categorized according to the WHO AWaRe classification, advocating for a preference in countries to utilize 60% of antibiotics from the ACCESS group for routine use. The progression from ACCESS to WATCH and RESERVE groups underscores the necessity for a measured escalation in antibiotic choice, emphasizing cautious selection over-enthusiasm, a principle that was also emphasized to students during the activity.
The card-based approach did not significantly outperform the lecture in final scores, likely due to the small sample size, its implementation in a single batch of students, and the limited exposure time to all the cards, despite the game being played three times. As the activity was newly introduced, students may not have had sufficient opportunity to fully engage with and internalize the material. It is possible that with increased repetitions, the card-based approach could yield better results than traditional didactic lectures, to which students are more accustomed. The card-based activity likely provided a more engaging and memorable learning experience, which might potentially lead to better long-term retention and application of knowledge, which was not captured in our immediate post-test assessment. Integrating the card-based activity into the antibiotic teaching curriculum as a recurring component, rather than a one-time intervention, would allow for the assessment of its impact on long-term retention and applied knowledge. A future study with a larger sample size and extended duration could provide more comprehensive insights into its effectiveness.
The majority of the students who found the card-based activity useful agreed (Figure 1) that the cards enhanced their understanding of the Antibiotic spectrum, toxicity, and unique attributes in terms of coverage or use for drug-resistant organisms. These students provided feedback such as ‘Very interesting way of learning about the complicated facts about the drugs’, ‘Hope many such interesting activities are incorporated into various topics’, ‘A well-appreciated effort...just realized how much I lag’, ‘It was very useful for me to learn the antimicrobial agents, I would like to have more sessions like this for other topics as well’, ‘I want Trump card activity for other topics’, ‘Very interesting way of learning about the complicated facts about the drugs’, ‘It was very useful for me to learn the antimicrobial agents.. I would like to have more sessions like this for other topics as well.’ There were a lesser few who felt, ‘Do cards after lecture immediately’, couldn’t remember all the mechanisms of actions at the end’.
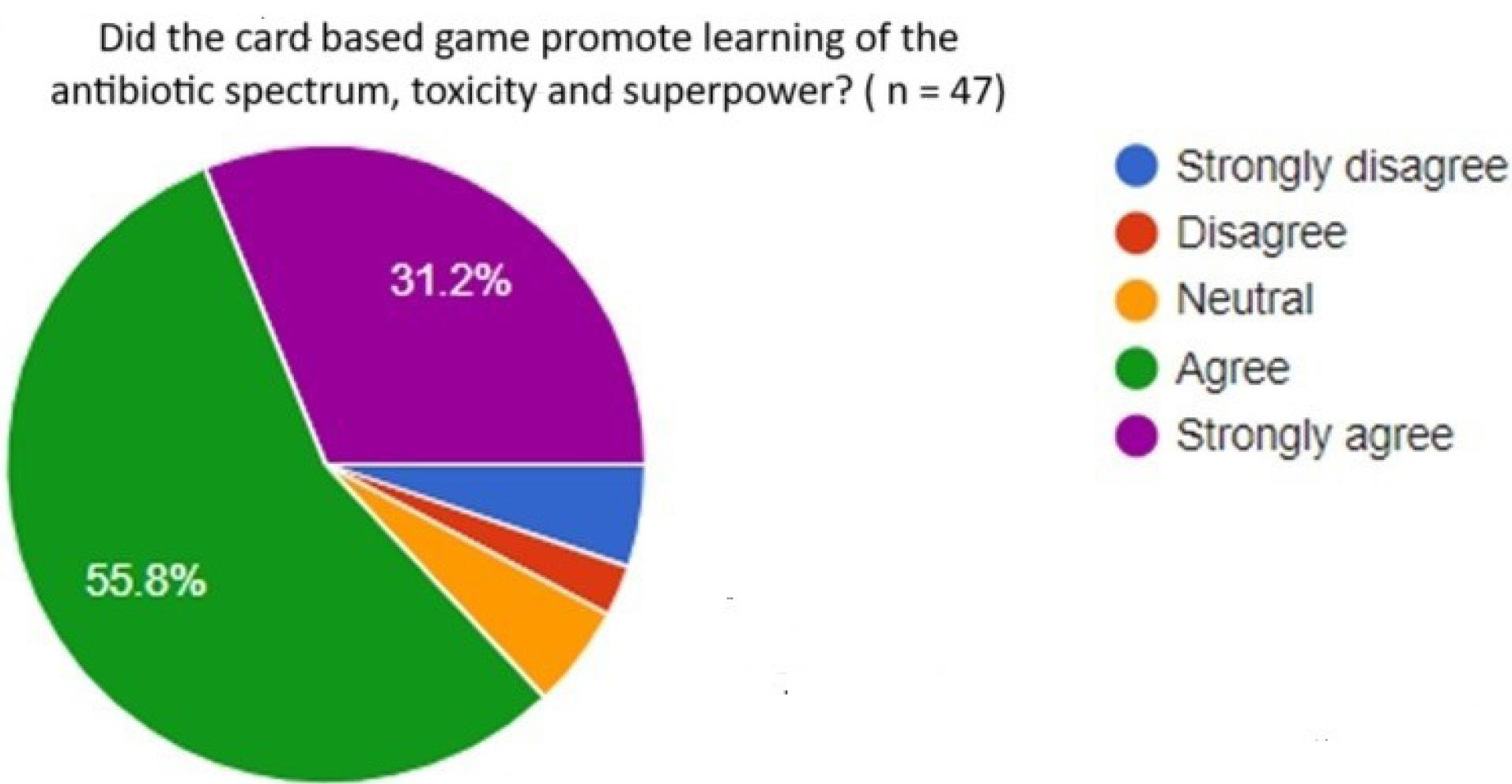
Figure 1.
Student feedback on the Effectiveness of the Card-based game
.
Student feedback on the Effectiveness of the Card-based game
The National Medical Council of India has reduced the number of teacher-centric didactic lectures and has allocated more hours to small group teaching and requires the undergraduate student to describe the Antibiotic Stewardship Programme of the institute.24
The positive response from students, many advocating for the extension of these interactive methods to other academic areas in pharmacology (Figure 2), highlights the broader potential of activity-based learning in medical education. While this approach may not supplant traditional didactic lectures, it could serve as a complementary or alternative method, enhancing the teaching of AMR awareness, rational antibiotic prescribing, understanding of uses, side effects, and application in drug-resistant infections. With projections indicating up to 8 million annual deaths attributable to AMR by 2050,25 every effort to mitigate these dreadful circumstances should be made especially for future clinicians and healthcare professionals.
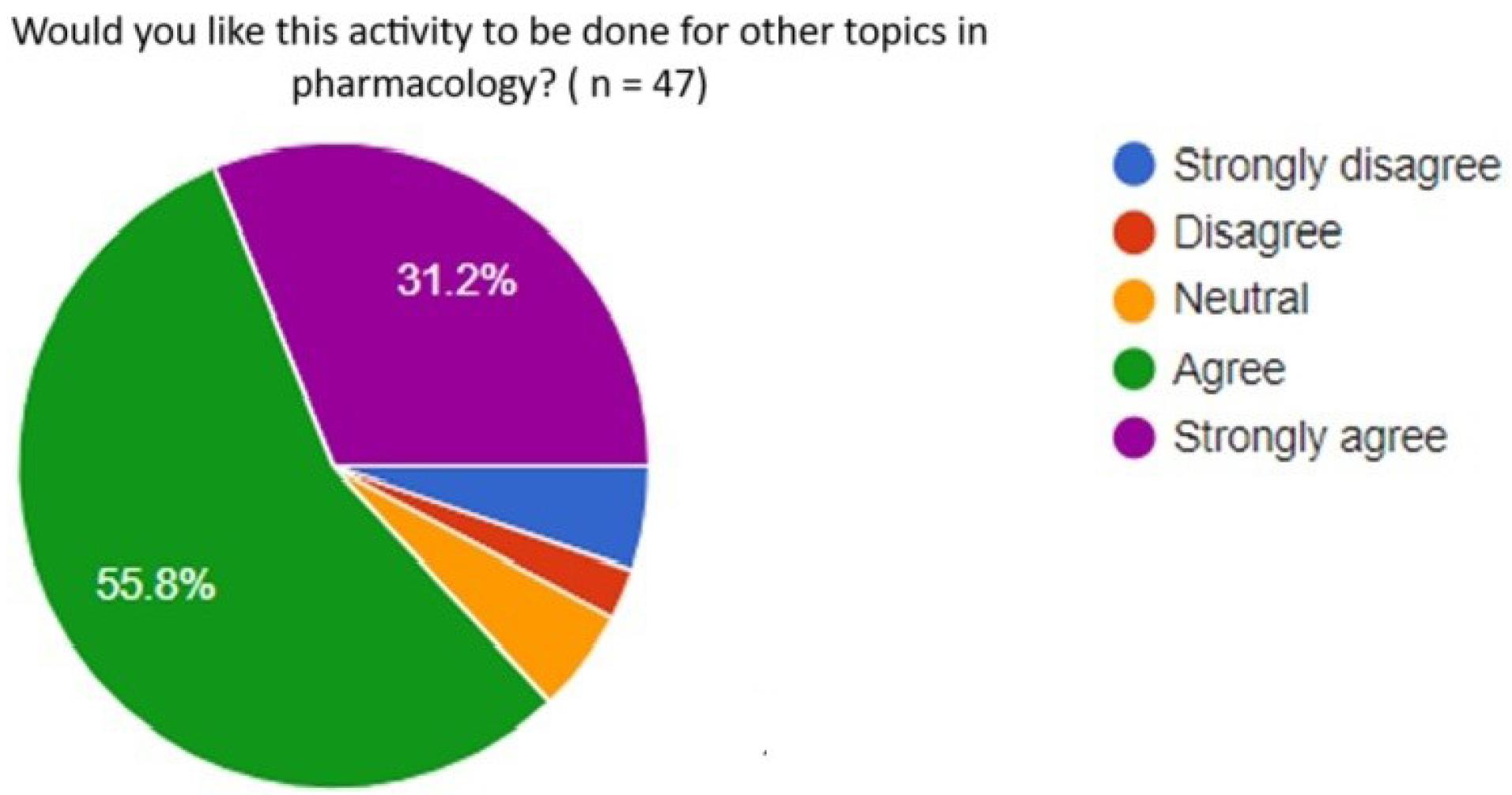
Figure 2.
Student feedback on expanding the activity to other topics in pharmacology
.
Student feedback on expanding the activity to other topics in pharmacology
Future directions could explore adapting this card game approach to other complex subjects and topics in medical education to enhance student engagement and knowledge retention. Additionally, scaling this method to larger cohorts across multiple institutions could provide broader insights into its efficacy and generalizability in diverse educational settings.
Limitations
The study’s single institution setting and small sample size of 100 students may limit the generalizability and statistical power of the findings. Potential selection bias could exist due to the homogeneous participant pool from one cohort. The limited exposure to the card game (three sessions) might not have been sufficient for long-term impact assessment. Future research should aim for a broader scope and larger sample to address these limitations.
Conclusion
The antibiotic-themed card game, though not statistically superior to traditional lectures in final test scores, offers significant educational value through enhanced engagement, highlighting its potential in medical education for teaching antimicrobial stewardship. The positive student feedback and the game’s ability to foster a deeper understanding of antibiotic use, resistance, and the importance of judicious prescribing underscore the value of interactive learning tools in preparing future clinicians to combat the global threat of antibiotic resistance effectively. These findings suggest implications for curriculum design, advocating for the integration of interactive, game-based learning into undergraduate medical education to complement traditional methods. To further explore the impact of this approach, future studies should assess its effect on long-term knowledge retention and application in clinical settings, ensuring that such innovative educational strategies can sustainably shape responsible antibiotic stewardship practices among healthcare professionals. Additionally, the scalability of this approach to other medical schools or topics presents an opportunity to enhance learning across various domains.
Competing Interests
The authors declare no conflict of interest.
Ethical Approval
Ethical approval was given by Instituional Review Board, Christian Medical College, Vellore, Institutional Review Board Approval Minute Number: 2407136, Date-24/7/2024 Christian Medical College, Vellore.
Acknowledgements
The authors express their gratitude to the Institutional Review Board for the fluid research grant, Christian Medical College, Vellore, and the faculties of the Department of Pharmacology, Christian Medical College, Vellore.
References
- Koya SF, Ganesh S, Selvaraj S, Wirtz VJ, Galea S, Rockers PC. Consumption of systemic antibiotics in India in 2019. Lancet Reg Health Southeast Asia 2022; 4:100025. doi: 10.1016/j.lansea.2022.100025 [Crossref] [ Google Scholar]
- Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf 2014; 5(6):229-41. doi: 10.1177/2042098614554919 [Crossref] [ Google Scholar]
- One Health Trust. Antimicrobial Resistance [Internet]. Available from: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance. Accessed November 25, 2024.
- Sulis G, Batomen B, Kotwani A, Pai M, Gandra S. Sales of antibiotics and hydroxychloroquine in India during the COVID-19 epidemic: an interrupted time series analysis. PLoS Med 2021; 18(7):e1003682. doi: 10.1371/journal.pmed.1003682 [Crossref] [ Google Scholar]
- Singh SK, Sengupta S, Antony R, Bhattacharya S, Mukhopadhyay C, Ramasubramanian V. Variations in antibiotic use across India: multi-centre study through global point prevalence survey. J Hosp Infect 2019; 103(3):280-3. doi: 10.1016/j.jhin.2019.05.014 [Crossref] [ Google Scholar]
- Machowska A, Landstedt K, Stålsby Lundborg C, Sharma M. Antibiotic prescribing to patients with infectious and non-infectious indications admitted to obstetrics and gynaecology departments in two tertiary care hospitals in central India. Antibiotics (Basel) 2020; 9(8):464. doi: 10.3390/antibiotics9080464 [Crossref] [ Google Scholar]
- Fazaludeen Koya S, Ganesh S, Selvaraj S, Wirtz VJ, Galea S, Rockers PC. Antibiotic consumption in India: geographical variations and temporal changes between 2011 and 2019. JAC Antimicrob Resist 2022; 4(5):dlac112. doi: 10.1093/jacamr/dlac112 [Crossref] [ Google Scholar]
- Pulcini C, Gyssens IC. How to educate prescribers in antimicrobial stewardship practices. Virulence 2013; 4(2):192-202. doi: 10.4161/viru.23706 [Crossref] [ Google Scholar]
- Luther VP, Shnekendorf R, Abbo LM, Advani S, Armstrong WS, Barsoumian AE. Antimicrobial stewardship training for infectious diseases fellows: program directors identify a curriculum need. Clin Infect Dis 2018; 67(8):1285-7. doi: 10.1093/cid/ciy332 [Crossref] [ Google Scholar]
- Silverberg SL, Zannella VE, Countryman D, Ayala AP, Lenton E, Friesen F. A review of antimicrobial stewardship training in medical education. Int J Med Educ 2017; 8:353-74. doi: 10.5116/ijme.59ba.2d47 [Crossref] [ Google Scholar]
- Abbo LM, Cosgrove SE, Pottinger PS, Pereyra M, Sinkowitz-Cochran R, Srinivasan A. Medical students’ perceptions and knowledge about antimicrobial stewardship: how are we educating our future prescribers?. Clin Infect Dis 2013; 57(5):631-8. doi: 10.1093/cid/cit370 [Crossref] [ Google Scholar]
- Schwartz BS, Armstrong WS, Ohl CA, Luther VP. Create allies, IDSA stewardship commitments should prioritize health professions learners. Clin Infect Dis 2015; 61(10):1626-7. doi: 10.1093/cid/civ640 [Crossref] [ Google Scholar]
- Charani E, Castro-Sanchez E, Sevdalis N, Kyratsis Y, Drumright L, Shah N. Understanding the determinants of antimicrobial prescribing within hospitals: the role of “prescribing etiquette”. Clin Infect Dis 2013; 57(2):188-96. doi: 10.1093/cid/cit212 [Crossref] [ Google Scholar]
- MacDougall C, Schwartz BS, Kim L, Nanamori M, Shekarchian S, Chin-Hong PV. An interprofessional curriculum on antimicrobial stewardship improves knowledge and attitudes toward appropriate antimicrobial use and collaboration. Open Forum Infect Dis 2017; 4(1):ofw225. doi: 10.1093/ofid/ofw225 [Crossref] [ Google Scholar]
- Trullàs JC, Blay C, Sarri E, Pujol R. Effectiveness of problem-based learning methodology in undergraduate medical education: a scoping review. BMC Med Educ 2022; 22(1):104. doi: 10.1186/s12909-022-03154-8 [Crossref] [ Google Scholar]
- Elendu C, Amaechi DC, Okatta AU, Amaechi EC, Elendu TC, Ezeh CP. The impact of simulation-based training in medical education: a review. Medicine (Baltimore) 2024; 103(27):e38813. doi: 10.1097/md.0000000000038813 [Crossref] [ Google Scholar]
- Gasim MS, Ibrahim MH, Abushama WA, Hamed IM, Ali IA. Medical students’ perceptions towards implementing case-based learning in the clinical teaching and clerkship training. BMC Med Educ 2024; 24(1):200. doi: 10.1186/s12909-024-05183-x [Crossref] [ Google Scholar]
- Davies AP. Evaluation of a novel antibiotic teaching resource. Med Sci Educ 2020; 30(1):107-9. doi: 10.1007/s40670-020-00927-y [Crossref] [ Google Scholar]
- World Health Organization (WHO). AWaRe Classification of Antibiotics for Evaluation and Monitoring of Use, 2023 [Internet]. Available from: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.04. Accessed November 25, 2024.
- National Medical Commission (NMC). National Action Plan on Antimicrobial Resistance. Available from: https://www.nmc.org.in/national-action-plan-on-antimicrobial-resistance/. Accessed April 8, 2025.
- World Health Organization (WHO). WHO Bacterial Priority Pathogens List, 2024: Bacterial Pathogens of Public Health Importance, to Guide Research, Development, and Strategies to Prevent and Control Antimicrobial Resistance. 1st ed. Geneva: WHO; 2024.
- Mogasale VV, Saldanha P, Pai V, Rekha PD, Mogasale V. A descriptive analysis of antimicrobial resistance patterns of WHO priority pathogens isolated in children from a tertiary care hospital in India. Sci Rep 2021; 11(1):5116. doi: 10.1038/s41598-021-84293-8 [Crossref] [ Google Scholar]
- World Health Organization (WHO). New Indian Priority Pathogen List to Guide Discovery of Effective Antibiotics [Internet]. Available from: https://www.who.int/india/news-room/detail/09-03-2021-new-indian-priority-pathogen-list-to-guide-discovery-of-effective-and-affordable-antibiotics. Accessed April 8, 2025.
- National Medical Commission (NMC). UG Curriculum. Available from: https://www.nmc.org.in/information-desk/for-colleges/ug-curriculum/. Accessed April 8, 2025.
- Naghavi M, Vollset SE, Ikuta KS, Swetschinski LR, Gray AP, Wool EE. Global burden of bacterial antimicrobial resistance 1990-2021: a systematic analysis with forecasts to 2050. Lancet 2024; 404(10459):1199-226. doi: 10.1016/s0140-6736(24)01867-1 [Crossref] [ Google Scholar]